














The purpose of this study was to compare the clinical and functional outcomes of anterior cruciate ligament reconstruction (ACLR) using hamstring tendon (HT) and bone–patellar tendon–bone (BTB) autografts through a prospective randomized trial. Thirty-eight patients with isolated ACL injuries were randomized to undergo ACLR using either HT (n = 19) or BTB (n = 19) autografts. All procedures were performed using an anatomic single-bundle arthroscopic technique. Patients were evaluated preoperatively and at 12 months postoperatively using the IKDC score, Rolimeter testing, Lachman and pivot shift tests, hop test, and range of motion. Both groups showed significant improvement in all parameters. The mean IKDC score was 82.6 ± 6.3 in the HT group and 83.2 ± 5.9 in the BTB group. No significant differences were found in knee stability, hop test results, or return-to-sport rates. No complications or graft failures occurred. ACLR using either autograft type yielded comparable outcomes. Graft choice should be individualized based on patient characteristics and surgeon preference.
Anterior cruciate ligament (ACL) injury is one of the most common and functionally disabling knee injuries encountered in orthopaedic practice, particularly among young and physically active individuals [1,2]. The ACL plays a vital role in maintaining knee stability by resisting anterior tibial translation and providing rotational control [3]. Untreated ACL injuries are strongly associated with functional instability, meniscal tears, chondral damage, and the development of early post-traumatic osteoarthritis [4,5].
Surgical reconstruction is the gold standard treatment for symptomatic ACL deficiency in active patients. The primary goal of anterior cruciate ligament reconstruction (ACLR) is to restore knee kinematics, allow safe return to sports, and prevent further intra-articular damage [6].
Among various graft choices for ACLR, the two most commonly used autografts are the bone–patellar tendon–bone (BTB) and the hamstring tendon (HT) grafts. Each graft has distinct biomechanical and clinical characteristics that influence the surgeon preference, selection and patient outcomes [7,8].
The BTB autograft type is often considered the “gold standard” because of its rigid bone-to-bone fixation and faster healing at the tunnel interfaces. Several biomechanical studies have confirmed its superior initial stiffness and load to failure [9,10]. However, this type of graft also associated with significant donor site morbidity including anterior knee pain, patellar tendinopathy, kneeling discomfort, and rare but serious complications like patellar fractures or tendon rupture [11,12].
On the other hand, the HT autograft type, typically harvested from the semitendinosus and gracilis tendons, which offers the advantage of lower donor site morbidity and reduced anterior knee pain. The graft is flexible also, which allows for smaller incisions, and may be biomechanically adequate when prepared as a quadrupled construct [13,14]. However, some studies reported increased postoperative laxity, slower graft incorporation due to soft-tissue-to-bone healing, and higher re-tear rates in certain athletic populations [15–17].
Numerous systematic reviews, including Cochrane and registry-based studies, have shown no definitive superiority of one graft type over the other with regard to patient-reported outcomes, knee laxity, or return to sports [7,18,19]. However, the major challenges in interpreting the literature stems from variations in surgical technique, rehabilitation protocols, and patient demographics.
In light of the ongoing debate and the absence of a clear consensus, this randomized controlled trial was designed to compare clinical and functional outcomes of ACLR using hamstring tendon versus bone–patellar tendon–bone autografts. Our hypothesis was that both grafts would yield equivalent stability and functional outcomes at one year follow up , which allowing for an evidence-based approach to personalized graft selection.
Materials and methodsStudy design and settingThis study was a prospective, randomized controlled trial conducted at Kasr Al-Ainy Medical School Hospital, Cairo University, Egypt between February 2020 and March 2022. Ethical approval was obtained from the Research Ethics Committee, Faculty of Medicine, Cairo University (Approval No CU-ORTHO-2020–043, dated January 20, 2020). A written informed consent was obtained from all patients prior to participation in the study. This study was not prospectively registered because institutional policy at the time of study initiation did not mandate registration for single-center investigator-initiated trials. Nevertheless, the trial was conducted according to CONSORT 2010 guidelines and all procedures followed the Declaration of Helsinki [20].
Randomization and blindingRandomization was performed in a 1:1 ratio using a computer-generated block sequence (block size = 4) created by an independent statistician.
Opaque, sequentially numbered sealed envelopes prepared by a study coordinator not involved in enrollment were opened intra-operatively immediately before graft harvest. Because the graft types differ, neither surgeons nor rehabilitation staff were blinded. All postoperative assessments were conducted by a senior physiotherapist blinded to group allocation and without access to operative notes. Objective outcome measures (Rolimeter, IKDC, hop test) minimized observer bias.
Patient selectionA total of 40 patients presenting with isolated ACL rupture were assessed for eligibility. After applying inclusion and exclusion criteria, 38 patients were enrolled to the study and randomized equally into two groups: 19 patients underwent ACLR using HT autografts, and 19 patients received BTB autografts. Baseline demographic and clinical data collected included age, sex, height, weight (used to calculate body mass index, BMI), dominant limb, symptom duration, sport type, and pre-injury activity level (Table 1).
Patient demographics and baseline characteristics.
p < 0.05 considered significant.
Our inclusion criteria were, patient age between 18 and 55 years, symptomatic, MRI-confirmed complete ACL tear, no radiological evidence of osteoarthritis > grade II (Kellgren-Lawrence), normal contralateral knee, and lastly patient willingness and ability to comply with rehabilitation and follow-up
Exclusion criteriaOur exclusion criteria were, patients with multiligamentous knee injury, complex meniscal root avulsions requiring additional major procedures, Previous surgery on the affected knee, contralateral knee pathology, systemic disease affecting healing (e.g., diabetes, rheumatoid arthritis), and active infection or open wounds.
Meniscal lesions identified at diagnostic arthroscopy were managed as follows: small, stable tears not requiring treatment were left in situ; tears requiring intervention (repair or partial meniscectomy) were treated at the time of ACLR and these patients were included in the study provided no other exclusion criteria were met. Patients with complex meniscal root avulsions requiring additional major procedures (e.g., root reconstruction) or multiligamentous injuries were excluded.
Surgical techniquesAll procedures were performed arthroscopically under spinal or general anesthesia by senior orthopedic consultants trained in sports surgery. Standard diagnostic arthroscopy was first conducted to confirm ACL rupture and rule out any additional intra-articular injuries.
Hamstring tendon group (HT)The semitendinosus and gracilis tendons were harvested through a small oblique incision over the pes anserinus. After tendons debridement and preparation, tendons were quadrupled and secured using whipstitch sutures. Anatomic single-bundle ACLR was performed. The femoral tunnel was drilled through the anteromedial portal with the knee in deep flexion (120°). Tunnel diameters were measured intraoperatively and recorded in millimetres. For hamstring grafts, the final graft diameter (quadrupled construct) was measured using a graft-sizing block and recorded. Both femoral and tibial fixation were achieved using BioComposite interference screw, Arthrex (Naples, FL, USA). The average screw diameters used were 7–8 mm; sizes were adjusted to match graft and tunnel diameters (Table 2).
Surgical technique and graft fixation characteristics.
p<0.05 considered significant.
A central-third BTB graft measuring approximately 10 mm wide and 25 mm long, with tibial and patellar bone plugs, was harvested through a longitudinal midline incision. Bone ends were shaped into trapezoids for anatomical fit. Tunnel placement was done similar to the HT group. Tunnel diameters were measured intraoperatively and recorded in millimeters. For BTB grafts, the minimum cross-sectional dimension of the tendon was recorded. Bone-to-bone fixation was achieved using BioComposite interference screw, Arthrex (Naples, FL, USA) of appropriate diameter. The average screw diameters used were 8–10 mm; sizes were adjusted to match graft and tunnel diameters. Special care was taken to minimize donor site morbidity.
All patients underwent the same arthroscopic technique for femoral and tibial tunnel preparation, graft passage, and tensioning (Table 2).
Postoperative rehabilitationA standardized rehabilitation protocol was followed in both groups, designed in accordance with current evidence-based guidelines [2,3]: Day 1–7: Isometric quadriceps activation, cryotherapy, and passive ROM 0–90°, week 2–6: Progressive weight bearing with crutches; closed-chain exercises; proprioception training, month 3: Jogging and low-impact sports-specific drills if quadriceps strength ≥ 80 % of contralateral limb, month 6–8: Return to full sport allowed if hop test and strength assessments ≥ 90 % symmetric
Patients were reviewed at 1, 3, 6, and 12 months postoperatively. Primary and secondary outcomes were recorded at baseline and final 12-month follow-up for analysis.
Statistical analysis and data interpretationSample sizeSample size was calculated using Power Analysis and Sample Size (PASS) software, version 15.0.5 for Windows (2017). The calculation was based on a minimal clinically important difference (MCID) of 10 points in the IKDC score [21]. as the primary outcome. Patients were allocated into two groups: Group I: BTB group, Group II: HT group. The null hypothesis assumed no difference between the two treatment modalities regarding the total postoperative IKDC score (non-inferiority design). A sample size of 17 patients per group was required to achieve 90 % power (1-β) using a one-sided two-sample unequal-variance t-test, with a margin of non-inferiority of 10 points and a significance level (α) of 0.05. To account for potential dropouts, 19 patients were enrolled per group, ensuring adequate statistical power.
Data analysisData analysis was performed by SPSS software, version 25 (SPSS Inc., PASW statistics for Windows version 25. Chicago: SPSS Inc.). Qualitative data were described using number and percent. Quantitative data were described using median (minimum and maximum) for non- normally distributed data and mean± Standard deviation for normally distributed data after testing normality using Kolmogrov-Smirnov test. Significance of the obtained results was judged at the (≤0.05) level.
- •
Chi-Square, Fischer exact test were used to compare qualitative data between groups as appropriate
- •
Mann Whitney U test were used to compare between 2 studied groups for non-normally distributed data.
- •
Student t-test was used to compare 2 independent groups for normally distributed data.
- •
Paired t-test was used to compare 2 paired readings for normally distributed data.
The primary outcome was the International Knee Documentation Committee (IKDC) subjective score at 12 months.
Secondary outcomes were ATT measured with a Rolimeter, Lachman test grade, single-hop test, Tegner activity score, and donor-site morbidity.
Anterior knee pain was assessed at each visit and documented as present or absent; no visual analogue scale (VAS) was used.
ResultsPatient enrollment and follow-upA total of 38 patients meeting inclusion criteria were randomized equally into two groups (19 HT and 19 BTB). All patients completed the minimum 12-month follow-up (100 % retention). There were no significant baseline differences in age, sex, BMI, symptom duration, or activity level between the groups (Table 1).
Surgical technique and fixationMean graft diameter was 8.4 ± 0.5 mm in the HT group and 10.0 ± 0.0 mm in the BTB group (p < 0.001).Femoral and tibial tunnels averaged 8.5 ± 0.6 mm and 8.6 ± 0.5 mm for HT versus 9.9 ± 0.3 mm and 10.0 ± 0.0 mm for BTB, respectively (both p < 0.001).
All fixations used BioComposite interference screws (Arthrex, Naples, FL, USA) of matching size (Table 2).
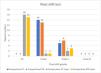
Anterior knee laxity (Rolimeter)Pre-operative ATT averaged 7.8 ± 1.2 mm (HT) and 8.0 ± 1.1 mm (BTB) (p = 0.54) (Fig. 1).

At 12 months, mean ATT improved to 2.3 ± 0.7 mm and 2.1 ± 0.8 mm, respectively, with no inter-group difference (mean Δ = 0.2 mm; 95 % CI −0.3 to 0.7; Cohen’s d = 0.27; p = 0.42) (Table 3).
Clinical stability – lachman and pivot shift testsLachman test at final follow-up, grade 0–1 stability was observed in 94.7 % (HT) and 100 % (BTB) (p = 0.31) (Fig. 2). No patient exhibited grade 2 or 3 laxity (Table 4).

Pivot Shift test (Grade 0/1):Negative/trace pivot shift: HT = 89 %, BTB = 95 %, P value = 0.3 (Table 4).
These results demonstrate equivalent graft stability at one-year follow-up (Figs. 2,3).
Functional outcomes
The mean IKDC subjective score improved significantly within both groups (pre-op ≈ 44 → post-op ≈ 83; p < 0.001 each) ( Fig. 4).

At 12 months, HT = 82.6 ± 6.3 (95 % CI 78.9–86.3) vs BTB = 83.2 ± 5.9 (95 % CI 79.6–86.8) (Δ = −0.6 [95 % CI −4.9 to 3.7]; Cohen’s d = 0.10; p = 0.80).
Hop-test performance reached 94.6 ± 4.2 % (HT) and 95.2 ± 3.8 % (BTB; p = 0.67).
Median postoperative Tegner level was 6 [IQR 5–7] in both groups (p = 0.91).
Lysholm scores were not systematically recorded and are therefore not reported (Table 5).
Functional outcomes – IKDC and hop test.
CI = confidence interval; SD = standard deviation; IKDC = International Knee Documentation Committee.Values expressed as mean ± SD unless stated otherwise. p < 0.05 considered significant. Cohen’s d: 0.2 = small, 0.5 = moderate, 0.8 = large effect.
Anterior knee pain occurred in 6 patients (31.6 %) of the BTB group and 2 (10.5 %) of the HT group (p = 0.11).
Kneeling pain was noted in 5 BTB and 1 HT patient (p = 0.08*).
There was 1 graft failure (BTB) and no infections or cyclops lesions.
Mean time to return to sport was 9.1 ± 1.6 months (BTB) and 8.8 ± 1.5 months (HT; p = 0.52).
Approximately 76 % of all patients resumed their pre-injury activity level (Fig. 5) (Table 6).

Return to sport and complications.
p < 0.05 considered significant.
No significant inter-group differences were detected for IKDC, ATT, hop test, Tegner level, or return-to-sport time.
Although anterior knee pain and kneeling discomfort were more frequent after BTB grafting, the differences did not reach statistical significance.
Both graft options achieved equivalent short-term clinical stability and functional recovery.
All clinical evaluations were performed by a blinded senior physiotherapist trained in orthopaedic outcome measurement.
DiscussionThis randomized controlled trial provides additional evidence that both HT and BTB autografts achieve comparable outcomes one year after ACLR. Both groups in our study demonstrated statistically significant improvements in knee stability, subjective knee function, and functional hop performance, with no significant differences between them.
This randomized controlled trial provides additional evidence that both HT BTB autografts achieve comparable outcomes one year after ACLR. Both groups in our study demonstrated statistically significant improvements in knee stability, subjective knee function, and functional hop performance, with no significant differences between them.
These findings are consistent with a Cochrane systematic review by Mohtadi et al. [7], which included 17 randomized controlled trials (RCTs) and concluded that both grafts offer similar outcomes in terms of stability and patient-reported function, although BTB grafts were associated with higher rates of anterior knee pain and kneeling discomfort. Similarly, a large-scale meta-analysis by Xie et al. [8] analyzing 47 studies found that BTB grafts provided slightly better stability but worse donor-site morbidity, reinforcing the concept that both grafts are clinically effective.
Although no anterior knee pain requiring intervention was observed in our series, long-term studies have reported persistent kneeling discomfort in up to 50 % of BTB graft recipients [22]. A 5-year follow-up RCT by Sajovic et al. [6] reported that both HT and BTB grafts led to excellent knee function, but BTB patients had higher rates of anterior knee pain and pain during kneeling (29 % vs. 7 %). Our study aligns with their short-term data and confirms the absence of superiority regarding stability or IKDC scores at 12 months.
Another long-term RCT by Pinczewski et al. [13], with a 10-year follow-up, showed that HT grafts had lower rates of kneeling pain and similar rates of graft failure and return to sport compared to BTB. However, they did observe slightly increased pivot shift positivity in the HT group — an effect not confirmed in our study, likely due to improvements in fixation methods such as suspensory devices and tunnel drilling techniques.
Adjunctive procedures, such as lateral extra-articular tenodesis, have recently gained attention for reducing residual pivot shift in high-demand patients, as demonstrated in the stability trial [23].
Our results also parallel those of the MOON (Multi-center Orthopaedic Outcomes Network) cohort [16], where no clinically significant difference was found between HT and BTB grafts in over 2000 patients. Notably, their study emphasized that surgeon experience and patient rehabilitation adherence had more influence on outcome than graft choice itself.
Return-to-sport rates were slightly higher in the BTB group (95 % vs. 89 %), though not statistically significant. Similar findings were reported by Ibrahim et al. [24] and Feller & Webster [25], who demonstrated no significant difference in activity resumption at mid-term follow-up. The importance of concomitant meniscal status on final outcomes was highlighted by the MARS Group [26].
In addition, rehabilitation strategies and neuromuscular training programs have been shown to play a crucial role in restoring functional performance and minimizing re-injury risk [27,28]. Anterior knee pain following BTB autograft harvest has been identified as a potential risk factor for delayed return to full athletic participation [29].
Recent literature also emphasizes the role of psychological readiness and fear-avoidance behaviors as critical factors affecting successful return to sport, beyond purely physical rehabilitation metrics [30].A major strength of our study is the uniformity in surgical technique and rehabilitation protocol. Unlike some prior RCTs that included multiple surgeons or varied rehab programs, our study eliminated these confounders. Moreover, we used validated functional tests such as the single-leg hop test and the IKDC subjective knee score, improving the reliability of our comparisons.
Study limitations must be acknowledged. The sample size is relatively small, limiting the power to detect rare complications or subtle differences. Furthermore, the follow-up duration was limited to 12 months; therefore, conclusions regarding long-term graft integrity, osteoarthritis development, or re-injury rates cannot be made. Additionally, donor-site morbidity was not quantitatively measured using VAS or anterior knee pain scales, which might have revealed functional trade-offs between graft types. Finally, meniscal pathology was not analyzed in depth because cases requiring repair were excluded; however, subtle ramp or root lesions may still influence long-term biomechanics.
Despite these limitations, the trial’s strengths include homogeneous surgical technique, single-surgeon consistency, standardized rehabilitation, and blinded outcome assessment — minimizing selection and performance bias.
Clinical interpretationThis study confirms that ACLR with either HT or BTB autografts can yield excellent short-term outcomes. Given the comparable clinical performance, the choice of graft should be tailored to the patient’s lifestyle, professional demands (e.g., occupations requiring kneeling), and preference—an approach supported by systematic reviews and multi center databases [6–10,15–16,19].
ConclusionBoth hamstring tendon and patellar tendon autografts offer reliable results at one year after ACLR.
Donor-site morbidity was slightly higher in the BTB group, though this did not affect overall function.
Given these comparable findings, graft selection should be personalized according to the patient’s sport demands, occupational activities, and preference, rather than any inherent superiority between graft types.
Our findings reinforce the concept that there is no absolute “gold standard” graft and that individualized decision-making should be emphasized.
Future research should aim to include large, multi-center randomized controlled trials with standardized surgical techniques and rehabilitation protocols, longer follow-up periods to evaluate graft survival and osteoarthritis progression, and more comprehensive assessment of donor-site morbidity and patient-reported outcomes. Such studies would provide higher-level evidence to guide graft selection and optimize long-term outcomes for diverse patient populations.
Item 1. Board member/owner/officer/committee appointments:____N/A______
Item 2. Royalties:___N/A_______
Item 3. Speakers bureau/paid presentations:___N/A_______
Item 4A. Paid consultant or employee:___N/A_______
Item 4B Unpaid consultant:___N/A_______
Item 5. Research or institutional support from publishers:___N/A_______
Item 6. Research or institutional support from companies or suppliers
(data generated from such studies must be unrestricted):__N/A_________
Item 7. Stock or stock options:___N/A_______
This study was approved by the Research Ethics Committee of the Faculty of Medicine, Cairo University. Written informed consent was obtained from all participants prior to their inclusion in the study.
Consent for publicationNot applicable.
Availability of data and materialThe datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
FundingThere is no funding source.
Authors’ contributionsAME: Conceptualization, Methodology, Project administration, Investigation, Supervision, Writing – original draft. WR: Investigation, Resources, Data curation. AMG: Formal analysis, Validation, Visualization. AES: Literature review (covered under Investigation), Writing – review & editing.All authors read and approved the final manuscript.
The authors declare that they have no conflict of interest.
Not applicable.

