









The objective of the study was to evaluate sleep, circadian rhythms and neurocognitive status of high performance athletes during the usual period of training, competitions and studies.
Materials and methodsA team of 12 high-performance basketball players (women, 15–17 years old) concentrated in a sports residence was evaluated. Sleep was studied through polysomnography, circadian rhythms using ambulatory circadian monitoring sensors, and neurocognitive status using s battery of questionnaires.
ResultsAthletes sleep 6:57±0.02h, nocturnal activity of 201.1±33.7% is above normal range (65–135%), regularity of schedules, 72.6±9.2% is also out of range (75–125%). The sleep depth of 85.1±2.6% (normal values between 85 and 100%) is reduced, and the peripheral temperature during the day, of 33.4±0.9°C (normal values between 31 and 33°C) indicates drowsiness.
ConclusionsOur sample of athletes sleep less than the necessary hours, their sleep quality is low due to muscle fatigue and poor habits, and their irregular schedule deteriorates the circadian system. All of this influences both physical and mental performance. It is essential to raise awareness of the importance of improving these sleep habits in order to maintain optimum physical performance.
El objetivo del estudio fue evaluar el sueño, ritmos circadianos y estado neurocognitivo de deportistas de alto rendimiento durante el periodo habitual de entrenamiento, competiciones y estudios.
Materiales y métodosSe evaluó un equipo de 12 jugadoras (mujeres, 15-17 años) de baloncesto de alto rendimiento, concentrado en una residencia de deportistas. Se estudió el sueño mediante polisomnografía, los ritmos circadianos mediante sensores de monitorización circadiana ambulatoria, y el estado neurocognitivo mediante batería de cuestionarios.
ResultadosLas deportistas duermen 6:57±0,02h, la actividad nocturna del 201,1±33,7% se sitúa por encima de la normalidad (65-135%), la regularidad de horarios, de un 72,6±9,2% también está fuera de rango normal (75-125%). La profundidad de sueño del 85,1±2,6% (valores normales entre 85-100%) es reducida, y la temperatura periférica elevada durante el día, de 33,4±0,9°C (valores normales entre 31-33°C) indica somnolencia.
ConclusionesLas deportistas de nuestro estudio duermen menos horas de las necesarias, la calidad del sueño es baja debido a la fatiga muscular y a unos malos hábitos, y los horarios irregulares deterioran el sistema circadiano. Todo esto influye en su rendimiento tanto físico como mental. Es básico concienciar al colectivo con todos los estamentos implicados, de la importancia de mejorar estos hábitos de sueño para mantener el rendimiento físico óptimo.
Scientific evidence proves that one of the main factors which influence sport performance is the quality and quantity of the hours during which sportsmen and sportswomen sleep.1
Sports development and performance are chiefly based on training, although other “invisible training” factors also play an important role. These include physical recovery, psychological preparation, nutrition and also rest. Correct sleep plays a highly important role in athletic performance and in physical, physiological and metabolic recovery, while it also ensures good cognitive condition and mood.
However, the discipline of those who do sports also leads to a reduction in their hours of sleep, problems with the quality of their rests and deterioration of their circadian rhythms.2–6 The hours of training, competitions and the stress and anxiety they cause, the high degree of physical wear and over-training all affect their rest. This wear and the poor quality of their sleep prevent the necessary physical repair from occurring, affecting physical and mental recovery.
Numerous studies have been published on how lack of rest affects physical recovery and performance. Skein et al.7 associate lack of sleep with a fall in the levels of muscular glycogen, and as a result of this with poorer performance in athletic competitions; VanHelder et al.8 emphasise the relationship between sleep loss with an increased metabolic demand and higher energy consumption. Likewise, recovery becomes less effective due to the increase in energy consumption and metabolic demand.9,10 Finally, lack of sleep has also been identified as the most important factor in the risk of suffering injuries, increasing the risk of injury 1.7 times, according to a study of 160 adolescent athletes.11
Circadian rhythms are genetically determined by the nature of each individual, and they will influence variations in performance throughout the day.12 It is very important to preserve the rhythm to conserve homeostatic balance, which is directly associated with mental and physical functions, cardiovascular working, core temperature or the metabolism. Training times should be tailored to the chronotype of each sportsman or sportswoman.
The influence of lack of rest is no less important in terms of mood and cognitive state. The perception of fatigue, resistance against stress, working capacity, reaction time and concentration are all affected by a lack of sleep.13
A work directly connected with this study was published by Mah et al.14 This studies the effect of length of sleep on the performance of a team of basketball players in Stanford University. The average length of sleep at first was 7h 45min, and this was extended to 9h 15min, after which significant improvements were observed in all athletic performance tests: subjects ran faster and displayed greater accuracy in free shots at the basket and triples, together with an improved subjective opinion of their athletic performance. Likewise, in different tests the players expressed lower levels of sleepiness (the Epworth test), a better mood profile, less fatigue and greater vitality (the POMS test), together with a fall in reaction time (PVT test).
This paper studies sleep in an elite women's basketball team. It does so to supply more scientific data on the quality and quantity of their rest. For the first time sleep is analysed objectively here by ambulatory circadian monitoring (ACM). This makes it possible for us to objectively analyse hours of sleep, its quality, waking up during the night, daily habits, body temperature and circadian rhythms, among other parameters. Additionally a battery of questionnaires was used to evaluate the neurocognitive conditions of the subjects.
The data obtained will make it possible to learn how many hours are slept as well as sleep quality. It will be possible to detect possible pathologies, evaluating sleep habits and environmental influence for good quality sleep.
Material and methodsAn observational study was undertaken of a high level basketball team of 12 players (women aged from 15 to 17 years old) (with the signed consent of their parents or tutors), who lived in a sports hall of residence (Residencia Blume, Esplugas de Llobregat). Each participant's sleep was studied by polysomnography during one night, in their usual rooms in the same hall of residence. Their circadian rhythms were also studied using chronobiological sensors which they wore like a watch for 24h a day during 7 days of habitual activity. Finally, a battery of questionnaires was used to evaluate the psychological and neurocognitive state of the participants.
PolysomnographyThe polysomnography recording (Clínica de Sueño Dr. Estivill, Barcelona) during one normal night in the subject's usual room (in the sports hall of residence), was performed to analyse the sleep structure of each participant and to detect possible sleep pathologies that could interfere with the nocturnal rest of the subjects (Apnea/Hypoapnea, regular limb movements or parasomnia).
Cerebral activity was recorded by contact electrodes, following the techniques set by the American Academy of Sleep. Electromyographic activity (EMG) was measured by applying electrodes to the area under the chin and the tibialis anterior muscles. A body position sensor was used. The heartbeat was also recorded. Eye movements (EOG) were measured by two electrodes placed close to the eyes. Nose and mouth thermal resistances were used with a pressure transducer, as were abdominal and thoracic induction strips were used to analyse respiratory dynamics. Nasal flow and blood oxygen saturation (SaO2) were measured by pulse oxymetry. PSG data were simultaneously acquired through 15 different channels at 30s per page during 8h.
Circadian study (ACM)The participants’ circadian rhythms and sleep/waking cycle were studied using a multichannel Ambulatory Circadian Monitoring (ACM) device (Kronowise®, Chronolab, Murcia University) that consists of: 1) a wristwatch that includes a temperature sensor (Thermochron® iButton DS1921H, Dallas, Maxim) to record distal body temperature (°C) as an indirect indicator of sleepiness,15 and an ambient temperature sensor (Hobo® PendantTemp/Light Data Logger) (°C) and light sensor (lx); 2) an actimeter (Hobo® Pendant G Acceleration Data Logger) as a bracelet which records acceleration (m/s2) and static position (°) in three axes to evaluate repose/activity rhythms.
The sensors were worn 24h per day for 7 days, with normal everyday habits. The variables of position, activity and light were recorded every 30s and body temperature was recorded every 10min.
All data were analysed by used Circadianware® (Chronolab, Murcia University) software, and the average was shown of individual body temperature, light and activity parameters over the 7 days, and they were then compared with the standard values of a normal population.
The algorithmic calculation of body temperature (T), motor activity (A) and position (P) gave the integrated variable TAP16 as the result, this being an estimation of the level of activation which makes it possible to infer periods of sleep or wakefulness. High TAP levels correspond to low body temperatures with high values of activity and position that represent periods with a high level of mental and physical activity (wakefulness). A low TAP level corresponds to high temperature levels and low levels of activity and position, which are typical sleep values.
Analysis of the data recorded by the sensors offers a range of indicators about sleep and circadian rhythms: hours of sleep, average temperature during the night as an indicator of depth of sleep, average temperature during the day as an indicator of wakefulness or sleepiness, activity during the night as an indicator of broken sleep and depth of sleep, regular habits to evaluate circadian rhythms, the interday stability (IS) associated with the regularity of the sleep/wakefulness cycle from one day to another, the intraday variation (IV) of the recorded variables, the relative amplitude (RA) of the contrast between variables during wakefulness and sleep, and the circadian working of the wakefulness/sleep cycle (CFI) as the overall indicator of the robustness of the circadian rhythms.
The battery of questionnairesThe participants completed the following battery of questionnaires: the subjective level of sleepiness was measured using the Epworth sleepiness scale (ESS),17 which runs from 0 to 24 and where 9 is the value showing maximum normality. The compound morningness scale (CMS)18 measured the chronotype or genetically determined profile for eveningness or morningness which conditions the physical performance of each sportsman and sportswoman at training times. The executive functions were evaluated using the TESEN Trails Test (Test de los Senderos TESEN (JA. Portellano, R. Martínez Arias, TEA ediciones, Madrid)), a standardised questionnaire derived from the TMT,19 that is based on the capacity for visual planning. The times taken are measured together with the number of errors committed.
The profile of mood states (POMS)20 was applied to determine 7 profiles: stress, depression, anger, vitality, fatigue, confusion and sociability. This tool is widely used in sports, where it is found that negative mood states are more reduced in value than is the case in the normal population, while vitality is higher.21 This profile, which is characteristic of those who do sports, follows the Iceberg model and is affected by overtraining and fatigue.22
ResultsThe average age of the study participants was 16±0.8 years old, with an average weight of 69±7.1kg, 185±6.1m in height and a BMI of 20.7±1.1.
According to the results of the CMS chronotype questionnaire 6 players were found to have a morning profile (with a score of from 36 to 55), 2 had an evening profile (a score of 13–26), while the others had an intermediate chronotype. The Epworth sleepiness scale gave a subjective sleepiness score of 9 (borderline normality), corresponding a 54% of the subjects with an excess of sleepy (with a score above 9). During the study, a high level of injuries was observed, affecting 75% of the participants.
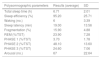
Polysomnography resultsThe polysomnographic studies detected one pathological record due to psychophysiological insomnia (case 1), one case of postural hypoapnea (case 6) and one case of excessive limb movements (myoclonus, case 12). The average values obtained in the 9 normal records are shown in Table 1: the sleep structure according to the percentages of the different phases of sleep are within normal limits, although the average total length of time slept was short, with a high level of sleep latency and an excessive number of arousals (or microwakings).
Average and standard deviation of polysomnographic parameters during the study of one night's sleep in the subjects with no associated pathology.
| Polysomnographic parameters | Results (average) | SD |
|---|---|---|
| Total sleep time (h) | 6.71 | 2.01 |
| Sleep efficiency (%) | 95.20 | 25.71 |
| Waking (no.) | 6 | 3.39 |
| Sleep latency (min) | 19.00 | 13.56 |
| Fragmentation (%) | 15.90 | 4.88 |
| REM (%/TST) | 23.90 | 7.28 |
| PHASE 1 (%/TST) | 3.70 | 1.78 |
| PHASE 2 (%/TST) | 48.10 | 13.60 |
| PHASE 3 (%/TST) | 24.60 | 7.06 |
| Arousal (no.) | 67 | 22.64 |
Daily recording over 7 days of the T, A, TAP, sleep and light variables supplied data on the number of hours they slept and the depth of their sleep. Their circadian rhythms of wakefulness and sleep depending on the regularity of their habits were also observed. The results were compared with those corresponding to a normal population by means of graphic representation of the weekly averages of the variables.
Fig. 1 shows an example of this type of record. The hours of sleep during different days are irregular due to poor habits. There is a high level of activity at the start of the night due to difficulty in falling asleep, and the high daytime temperature is an indication of sleepiness.

(A) Diagram showing the placement of the ambulatory circadian monitoring sensors. (B) Example of graphic representation of the 7-day chronobiological study. Left: graphic representation of the weekly average of the TAP, temperature, physical activity, sleep and light variables (coloured areas), compared with the standard values for the healthy population (blue lines). Right: graphic representation of the activity (blue), position (green) and temperature (red line) variables of an individual, recorded during 7 days. The estimation of sleep duration marked by the yellow strip is characterised by high temperature, a fall in movements and a low position. Episodes of waking during sleep are characterised by movements in position and a fall in temperature.
Table 2 shows the results of the circadian studies of all the participants together with the average of each one of the parameters that were calculated. In general it was observed that the number of hours slept during the whole week (7:35h) is less than is necessary given the participants’ age, and they sleep even less when only weekdays are considered (6:55h). This is associated with the sleepiness they suffer during the day, as detected by their generally raised temperature (daytime temperature: 33.38°C) compared with the normal value in a range of 31–33°C. Excessive activity during the night was also detected (201.09%), compared with normal values (65%–135%). This was due to broken sleep that gave rise to sleep that was not very refreshing. Finally, regularity of habits (72%) and depth of sleep (84.94%) are both lower than normal in a healthy population (75%–125% and 85%–100%, respectively). These alterations are associated with a certain degree of disruption in their circadian rhythms.
Results of the parameters (normal values are bracketed) of the record of the circadian study during one week of each one of the subjects (blank spaces in the data are due to measurement errors). The bottom shows the average and standard deviation.
| Hours sleep | Sleep weekdays | Regular habits (75–125%) | Daytime T (31–33°C) | Night-time T (34–36°C) | Night activity (65–135%) | Depth of sleep (85–100%) | |
|---|---|---|---|---|---|---|---|
| 1 | 7:36 | 6:44 | 60.56 | 33.54 | 34.84 | 210.70 | 81.22 |
| 2 | 7:41 | 7:00 | 70.03 | 219.03 | 83.44 | ||
| 3 | 7:09 | 7:15 | 89.32 | 33.98 | 35.15 | 153.70 | 89.26 |
| 4 | 8:03 | 7:33 | 71.05 | 33.60 | 35.40 | 136.13 | 85.30 |
| 5 | 7:33 | 7:08 | 61.92 | 32.24 | 34.56 | 178.53 | 83.44 |
| 6 | 7:14 | 6:24 | 70.88 | 34.12 | 35.66 | 217.32 | 87.06 |
| 7 | 7:52 | 7:59 | 90.06 | 33.78 | 35.70 | 248.79 | 88.38 |
| 8 | 7:44 | 6:06 | 72.08 | 213.42 | 83.01 | ||
| 9 | 7:29 | 6:45 | 63.11 | 34.41 | 35.55 | 180.74 | 81.17 |
| 10 | 7:45 | 6:42 | 74.65 | 31.53 | 34.17 | 211.70 | 87.27 |
| 11 | 7:44 | 7:12 | 70.46 | 33.75 | 35.07 | 198.16 | 84.36 |
| 12 | 7:15 | 6:23 | 69.87 | 32.84 | 34.44 | 244.81 | 85.31 |
| Average | 7:35 | 6:55 | 72.00 | 33.38 | 35.05 | 201.09 | 84.94 |
| SD | 0:16 | 0:31 | 9.33 | 0.90 | 0.54 | 33.75 | 2.65 |
Table 3 shows other parameters which indicate the circadian functioning of the recorded variables. Low levels of the IS parameter (the regularity index) indicate that the temperature, TAP and sleep variables do not remain stable from day to day throughout the week, due to poor circadian habits. The same can be concluded from the low values of the CFI parameter, which reflects the poor circadian quality of their timetables. The high IV values show instability of the variables over 24h, indicating broken sleep. The relative amplitude (RA) of the temperature variable is low, due to the lack of difference between daytime temperature (that is abnormally high because of sleepiness) and the night-time temperature.
Average of the results of the parameters that characterise circadian rhythms over the recorded variables (T, TAP and Sleep) of the subjects. Normal limits are shown in brackets between the limiting and optimum values.
| Variables | T | TAP | Sleep |
|---|---|---|---|
| IS (interday stability) | 0.42 (0.4–1) | 0.48 (0.5–1) | 0.72 (0.6–1) |
| IV (intraday fragmentation) | 0.21 (0.21–0) | 0.43 (0.4–0) | 0.16 (0.1–0) |
| IA (interday amplitude) | 0.025 (0.22–1) | 0.58 (0.5–1) | |
| CFI (circadian rhythm) | 0.44 (0.46–1) | 0.61 (0.6–0.9) |
The length of time they sleep is completely determined by their activities and obligations during the week. We saw in Fig. 2 how they sleep for less time during the week, getting up very early to train while still going to bed late, preventing them from sleeping for as long as they need. On the other hand, at the weekend their wakefulness/sleep rhythm was generally found to become delayed, leading to a lack of synchronisation between their circadian rhythm at the weekend and during the week, a phenomenon known as social jet-lag.
The results of the battery of questionnaires
The questionnaire about mood states (POMS) gave results that are comparable with the Iceberg profile that is typical of elite sportsmen and sportswomen. The results shown by the average curve for these sportswomen (Fig. 3) show excessively high stress levels, depression, confusion and fatigue, together with a fall in vitality.

The chronic sleep deficit suffered by the participants may lead to the mood instability they display, and it is also associated with a lack of physical recovery.
The average results of the questionnaire on executive functions (TESEN) were correct in terms of execution and speed, in the 85% and 90% percentiles, respectively. Nevertheless, the average score for precision, in the 30% percentile, is normal-low. This is associated with insufficient mental flexibility, excessive impulsiveness and difficulties in working memory, mixed with emotional and motivational factors.
DiscussionBased on the polysomnographic study, circadian monitoring during one week and the battery of questionnaires, we are able to draw certain conclusions on the sleep of these players, their habits, circadian rhythms, quality of rest and the results of these for their sleepiness and mood.
Sportsmen and women of the age of the group studied need to sleep for at least 9h a night. However, we found that their training and study timetables hindered them from sleeping for the necessary time. They generally suffer a chronic lack of sleep that becomes highly exacerbated on working days. Although they try to recover at weekends, they go to bed later then and give rise to a desynchronisation of their circadian rhythm.
We also detected poor sleep quality. They are excessively active during sleep, and this may be due to the muscle fatigue accumulated during the day. This leads to broken sleep that is not refreshing. Additionally the hall of residence environment with its shared rooms and spaces prevents absolute silence and darkness during the night, which in turns leads to a delay in going to bed. Sleep routines and habits are affected by the social environment and timetable variations. Desynchronised circadian rhythms contribute to maintaining the sleep disturbances observed.
Lack of sleep and the poor quality of the same lead to daytime sleepiness, as shown by an excessively high temperature. This in turn may lead to poorer performance than would be expected of these sportswomen. We found that their mood was affected by fatigue, which affected the emotional control of the players in the team.
Scientific evidence shows the importance of maintaining hours of sleep as well as sleep quality for those who do sports. It should be considered a part of their invisible training, as it is necessary for them to achieve the physical recovery they require to maintain optimum sport performance as well as good emotional and cognitive stability. Good quality sleep is a necessity, with a stable timetable and good sleep routines, together with a favourable environment to ensure the quality of rest.
Nevertheless, the lack of sleep in the group of sportswomen studied shows that it is necessary to include strategies to improve in this area. Sleep deficiencies have in fact been observed beforehand in sportsmen and women in different sports. It is fundamentally important that everyone involved in sports training be aware of the necessary importance of night-time rest. The sleep and the physical and mental state of sportsmen and women have become degraded, so that, as published studies state, this correlates with poorer performance in sport and an increase in the probability of injuries. Sleeping for longer is therefore a fundamental condition for improving their performance.
Conflict of interestAuthors declare that they don’t have any conflict of interests.

