






studies on eccentric training with blood flow restriction (BFR) still has gaps, especially in strength and muscle hypertrophy. Therefore, this study aimed to analyze and compare the effects of six weeks of eccentric training of knee extensors at different load associated or not with BFR on strength, hypertrophy, and performance of knee extensors.
Methods61 men, healthy and untrained, performed six weeks of quadriceps muscle eccentric training in isokinetic dynamometer were randomized into four groups: high-load eccentric training with BFR (HLET-BFR), low-load eccentric training with BFR (LLET-BFR), high-load eccentric training (HLET) and low-load eccentric training (LLET). The strength, muscle structure and performance outcomes were evaluated at baseline, after 3 and 6 weeks of training.
Resultsfor eccentric peak torque in the first three weeks, HLET was superior to LLET, but similar to LLET-BFR. In the final three weeks, superiority was observed in relation to LLET-BFR; however, there was no difference in relation to HIET-BFR. For the outcomes isometric and concentric peak torque, muscle structure and performance, there were no differences between groups.
Conclusioneccentric training led to strengthening of knee extensors and improved performance, but without altering the muscle structure. LLET-BFR promoted gains similar to HLET in the first three weeks of training.
Although strength training programs generally involve carrying out actions during concentric and eccentric muscle contractions, the advantages of programs that use eccentric overload have been widely evidenced in the literature, predominantly when referring to increased strength, but also reflected in increased muscle mass.1-3
It has been proposed that the mechanical stimulus is the main mechanism responsible for the adaptations promoted by eccentric contractions.2 Regarding molecular and neural characteristics, it was concluded that eccentric training can benefit performance through favorable adaptations in physical function (strength, power, rate of force development, and stiffness), morphological adaptations (tendon and cross-sectional area of muscle fibers), neuromuscular adaptations (rapid rate of recruitment and firing of motor units), and performance (vertical jump, starting speed, and change of direction) in relation to concentric, isometric, and traditional training (eccentric/concentric).2 Due to the favorable adaptations, eccentric training has received considerable attention2 and has been studied as an interventionist strategy aimed at improving performance, preventing injuries, and rehabilitation.3
Other lines of evidences suggest that metabolic stress, resulting from the accumulation of metabolites, especially lactate and H+, represents drives muscle hypertrophy and may explain structural and functional adaptations in the absence of significant muscle tension (defined as training loads below approximately 60 % 1RM [one-repetition maximum]).4 Support for this assumption comes from studies in which metabolic stress is artificially increased by blood flow restriction (BFR). This type of training has been shown to induce gains in mass and strength in the muscles trained at low loads of approximately 20 % 1RM.5
Taken together, as both eccentric exercises and BFR training have been shown to be effective training modalities to facilitate gains in strength and muscle mass, albeit by different physiological mechanisms, it seems plausible that the combination of both modalities would offer additional benefits to its practitioners. Thus, in order to better clarify the impact of BFR during eccentric contractions, the present study aimed to analyze and compare the effects of high and low-load eccentric training associated with BFR (HLET-BFR and LLET-BFR) with high and low-load eccentric training without BFR (HLET and LLET) on strength, hypertrophy, and performance of knee extensors.
The hypothesis of the study is that LLET-BFR presents similar gains in strength, hypertrophy and performance compared to HLET; that HLET-BFR is superior compared to HLET and LLET-BFR and that HLET-BFR, HLET, LLET-BFR are superior to LLET.
MethodsParticipants and designThis is a randomized controlled clinical trial, with four parallel arms, simple-blind, with balanced randomization (1:1:1:1) and intention-to-treat analysis. All procedures were previously approved. All participants were asked to read and sign a consent form. The study follows the CONSORT 2010 statement checklist (Consolidated Standards of Reporting Trails) [Supplementary File 1], so that the information and quality of reports of interventions are well described. All participants were asked to read and sign a consent form. The protocol of the study was registered with Clinicaltrials.gov (NCT03601104).
The study sample consisted of male participants, healthy and untrained, aged between 18 and 35 years. Participants were recruited through pamphlets, online media, personal invitation and the database registered in the research laboratory. The sample size was estimated based on the results of the eccentric peak torque in the study by Baroni et al.6 considering a clinically relevant difference of 28.8 Nm to be detected, with a standard deviation of 24.0 Nm. Using a two-tailed hypothesis test with 80 % power and 5 % significance level, at least 12 individuals per group were required.
The inclusion criteria were: not having medical restrictions for the practice of resistance exercise; not being involved in lower limb strength training program during the three months prior to participating in the study; not being diagnosed with any metabolic, endocrine, cardiovascular, and/or respiratory disease; not being an alcoholic, using drugs and smoker; absence of a history of knee surgery or musculoskeletal injury of the dominant lower limbs or spine; not using ergogenic supplements to improve physical performance and/or muscle mass; and absence of one or more risk factors predisposing to thromboembolism.7
The exclusion criteria were: individuals who presented an episode of musculoskeletal injury during exercise that prevented its continuation; and not properly understanding the execution of the eccentric exercise.
Randomization and blinding processGroups were randomized by an individual who was unaware of the study design through generation of a randomly ordered list of allocation codes using online program (https://www.random.org). To hide the allocation list, randomization codes were placed in sealed and opaque envelopes numbered consecutively. Researchers involved in the training sessions did not participate in the evaluation sessions and researchers responsible for the evaluations did not follow the training sessions. Due to the nature of the intervention participants were not blinded.
Study designData collection was carried out at the Center for Studies and Assistance in Physiotherapy and Rehabilitation of FCT/UNESP between February 2018 and December 2018 in a temperature controlled (24 °C) room between 5 and 10 pm. Before the procedures, anthropometric characteristics were measured using a scale (Tanita BC 554, Iron Man/Inner, Arlington Heights Illinois, USA) and a stadiometer (Sany - American Medical do Brasil, São Paulo, Brazil).
In the first week, the participants performed three familiarization sessions with peak torque training and tests. In the second week, the participants underwent assessment of strength, muscle structure, performance and BFR measures. This was followed by a period of three weeks of eccentric training. In the sixth week, an intermediate evaluation of all the initially evaluated outcomes was performed. Subsequently, the participants performed a further three weeks of eccentric training and one week after the end of the training, the final evaluation of all outcomes was performed. All measurements were taken at the same time of day and under the same conditions for all participants (Fig. 1).
Eccentric training program
The eccentric training groups were HLET with 80 % of eccentric peak torque; LLET with 40 % of eccentric peak torque; HLET-BFR with 80 % of eccentric peak torque; and LLET-BFR with 40 % of eccentric peak torque. The participants performed six weeks of an eccentric training program comprised three sessions per week of the knee extensor dominant muscle, performed on the isokinetic dynamometer (Biodex System 3, Biodex Medical System, USA).8
The eccentric training performed in isokinetic aimed to isolate the eccentric contraction, but not exposing the volunteer to a level of muscle damage, as was done in the study protocol by Machado et al.9
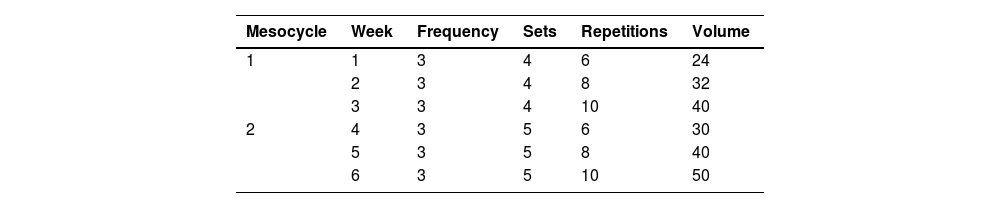
The training program was divided into two mesocycles, and the volume of the training session was increased in each mesocycle. The first (first three weeks) was composed of 4 series, in which the 1st, 2nd and 3rd weeks were performed 6, 8 and 10 repetitions, respectively and the second (last three weeks) was composed of 5 series and the 4th, 5th and 6th training weeks were also performed 6, 8 and 10 repetitions, respectively (Table 1). Each training session consisted of an isokinetic warm-up [6], followed by training with a one-minute rest period between sets.6,10
Eccentric contractions were performed with the individuals positioned on the dynamometer chair with 85° of hip flexion and 90° of knee flexion and were encouraged to perform knee extensor contraction at an angular speed of 60°/s as soon as the dynamometer arm reached the knee flexion position of 30° and a horizontal line in the monitor was added corresponding to the load of each participant.6,10,11
The eccentric torque peak was considered to define the percentage of training load of each participant, that is, 80 % and 40 % of the eccentric torque peaks of the results found in the evaluation.
In the groups that used BFR the cuff was positioned proximally to the thigh12 and inflated to 40 % of its absolute occlusion pressure (AOP) and was maintained throughout the exercise session and rest periods. The 40 % AOP restriction was chosen because studies show positive effects on the outcome of muscle strength and thickness with training load of 40 % 1RM7 and to avoid the deleterious effects on endothelial function, it is recommended that 40–60 % of BFR in training protocols.
Determination of blood flow restriction pressureParticipants remain seated and at rest for about 10 min.12 The transducer of the Doppler equipment (DV-2001; Medpej, Ribeirão Preto, São Paulo, Brazil) was positioned over the posterior tibial artery to capture the auscultatory pulse. To determine the AOP, a blood pressure cuff (cotton, velcro, 175 mm wide and 920 mm long, JPJ - hospital supplies industry, São Paulo, Brazil) was fixed and inflated in the proximal region of the participant's thigh.12 The cuff was progressively inflated until the auscultatory pulse was completely interrupted.13
Muscle strength assessmentIsometric, eccentric, and concentric peak torque were measured with an isokinetic dynamometer (Biodex System 4 Pro, New York, USA).11 Participants were previously instructed to perform all peak torque assessments with the greatest possible effort to develop maximum knee extension and verbal encouragement was provided during the tests.11 The highest peak torque values obtained during contractions was used for analysis.
Assessment of muscle structureUltrasound images of the dominant lower limb were captured using a Siemens ultrasound (Issaquah, WA, USA) Sonoline Sienna, together with a linear matrix transducer (48 mm, 7.5 MHz) to determine muscle thickness, angle of pennation, and fascicle length of the vastus lateralis (VL) and rectus femoris (RF) muscles.
Three images were collected from each muscle and analyzed using Image-J software (National Institute of Health, USA).10 The mean values obtained from the three ultrasound images of each muscle were used for analysis.
Assessment of performancePerformance was assessed using the Single Leg Hop Test.3 Participants were instructed to jump as far as possible, only on the dominant lower limb, starting from a static semi-squat position and to remain in a static position again after the jump. Participants performed up to five attempts, with minimum intervals of 30 s between attempts. For the jumps to be considered successful, the landing must be held for 2 s and the participants could not: touch the contralateral leg on the floor, touch both upper limbs on the floor, lose balance or perform an additional jump on landing. The mean of two well-executed hops was used for analysis, measured by a tape measure fixed to the ground.3
Statistical analysisFor analysis of the data of the sample profile, the descriptive statistical method was used and the results are presented with values of means, standard deviations, and confidence interval. The normality of the data was assessed using the Shapiro-Wilk test.
The comparisons of the outcomes between the four groups studied (HLET, LLET, HLET-BFR, and LLET-BFR) and the moments (baseline, intermediate, and final evaluation) were performed using two-factor repeated measures analysis of variance, which provided information on the effects of moment, group, and interaction. The repeated measurement data were checked for sphericity violation using the Mauchly's test and the Greenhouse-Geisser correction was used when the sphericity was violated. For moment analysis, Bonferroni's post-test for parametric distribution or Dunnett's post-test for non-parametric distribution was used and the analysis between the groups was performed using One-Way ANOVA or the Kruskal Wallis test.
In addition, training effects were verified for all outcomes assessed by calculating the effect size (ES) using Cohen's d, considered as “null” (<0.2), “small” (≥ 0.2), “moderate” (≥0.6), “large” (≥1.2), or “very large” (≥2.0).14 The level of significance was p < 0.05 for all tests. All analyses were performed with the statistical program SPSS (version 13.0) (SPSS Inc., Chicago, IL, USA) and followed the intention-to-treat principle.
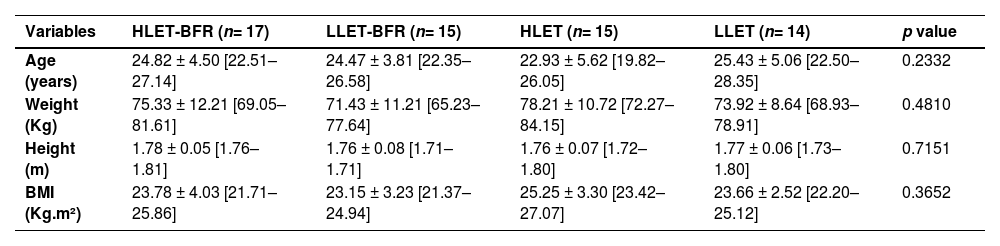
ResultsThe characterization of the studied sample is shown in Table 2. There were no statistically significant differences in relation to age, height, weight, and BMI. Among the 69 participants assessed for eligibility, eight were excluded because they refused to participate in the study. The detailed flowchart is shown in Fig. 2.
Subjects’ characteristics.
Values presented as mean ± SD [95 % confidence interval].
HLET-BFR: high-load eccentric training associated with blood flow restriction; LLET-BFR: low-load eccentric training associated with blood flow restriction; HLET: high-load eccentric training; LLET: low-load eccentric training; m: meter; Kg: kilogram; Kg.m²: kilogram square meter.

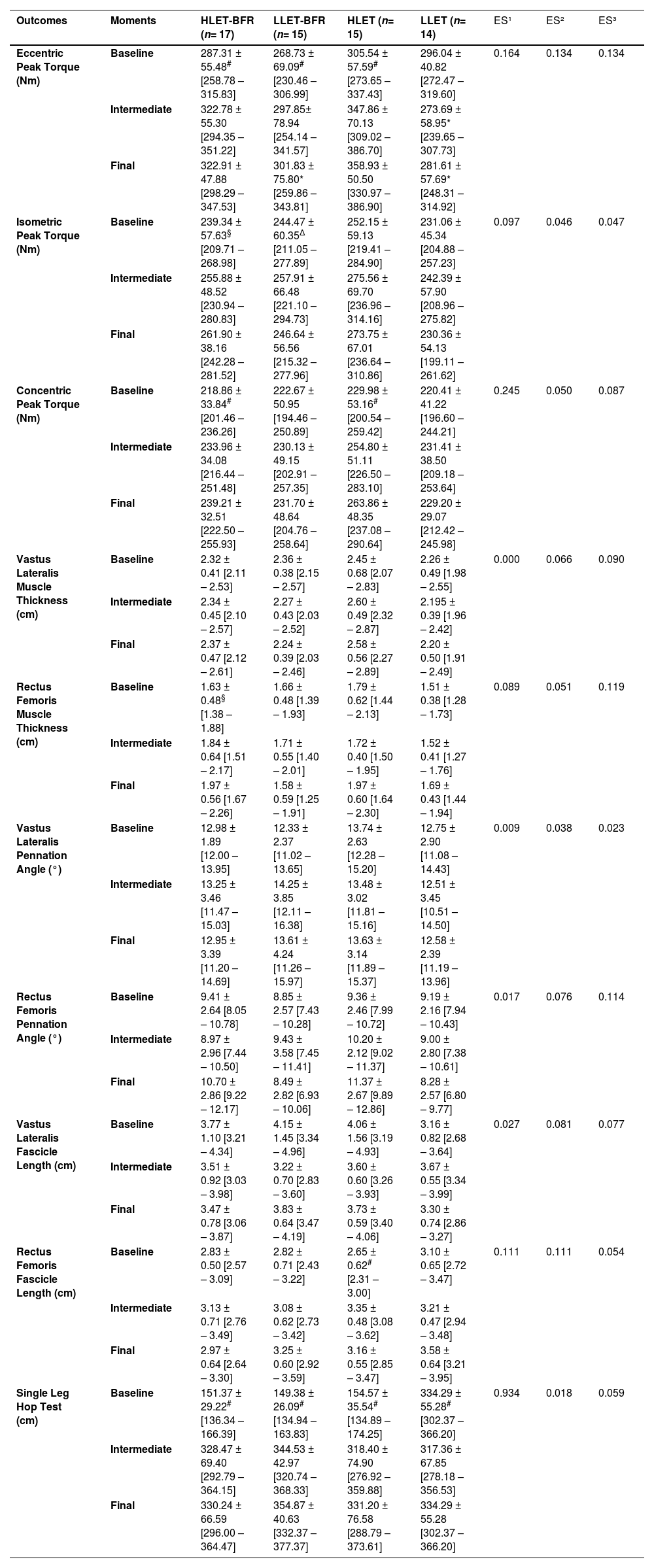
Table 3 shows the results of eccentric, concentric, and isometric peak torque, thickness, pennation angle, and fascicle length of the vastus lateralis and rectus femoris muscles, and performance at the baseline, intermediate, and final moments. Figs 3 and 4 show the percentage of changes found in the groups studied.
Outcomes of eccentric, isometric and concentric peak torques; muscle thickness, pennation angle and fascicle length of the vastus lateralis and rectus femoris and Single Leg Hop Test at baseline, intermediate and final moments of the studied groups.
| Outcomes | Moments | HLET-BFR (n= 17) | LLET-BFR (n= 15) | HLET (n= 15) | LLET (n= 14) | ES¹ | ES² | ES³ |
|---|---|---|---|---|---|---|---|---|
| Eccentric Peak Torque (Nm) | Baseline | 287.31 ± 55.48# [258.78 – 315.83] | 268.73 ± 69.09# [230.46 – 306.99] | 305.54 ± 57.59# [273.65 – 337.43] | 296.04 ± 40.82 [272.47 – 319.60] | 0.164 | 0.134 | 0.134 |
| Intermediate | 322.78 ± 55.30 [294.35 – 351.22] | 297.85± 78.94 [254.14 – 341.57] | 347.86 ± 70.13 [309.02 – 386.70] | 273.69 ± 58.95* [239.65 – 307.73] | ||||
| Final | 322.91 ± 47.88 [298.29 – 347.53] | 301.83 ± 75.80* [259.86 – 343.81] | 358.93 ± 50.50 [330.97 – 386.90] | 281.61 ± 57.69* [248.31 – 314.92] | ||||
| Isometric Peak Torque (Nm) | Baseline | 239.34 ± 57.63§ [209.71 – 268.98] | 244.47 ± 60.35∆ [211.05 – 277.89] | 252.15 ± 59.13 [219.41 – 284.90] | 231.06 ± 45.34 [204.88 – 257.23] | 0.097 | 0.046 | 0.047 |
| Intermediate | 255.88 ± 48.52 [230.94 – 280.83] | 257.91 ± 66.48 [221.10 – 294.73] | 275.56 ± 69.70 [236.96 – 314.16] | 242.39 ± 57.90 [208.96 – 275.82] | ||||
| Final | 261.90 ± 38.16 [242.28 – 281.52] | 246.64 ± 56.56 [215.32 – 277.96] | 273.75 ± 67.01 [236.64 – 310.86] | 230.36 ± 54.13 [199.11 – 261.62] | ||||
| Concentric Peak Torque (Nm) | Baseline | 218.86 ± 33.84# [201.46 – 236.26] | 222.67 ± 50.95 [194.46 – 250.89] | 229.98 ± 53.16# [200.54 – 259.42] | 220.41 ± 41.22 [196.60 – 244.21] | 0.245 | 0.050 | 0.087 |
| Intermediate | 233.96 ± 34.08 [216.44 – 251.48] | 230.13 ± 49.15 [202.91 – 257.35] | 254.80 ± 51.11 [226.50 – 283.10] | 231.41 ± 38.50 [209.18 – 253.64] | ||||
| Final | 239.21 ± 32.51 [222.50 – 255.93] | 231.70 ± 48.64 [204.76 – 258.64] | 263.86 ± 48.35 [237.08 – 290.64] | 229.20 ± 29.07 [212.42 – 245.98] | ||||
| Vastus Lateralis Muscle Thickness (cm) | Baseline | 2.32 ± 0.41 [2.11 – 2.53] | 2.36 ± 0.38 [2.15 – 2.57] | 2.45 ± 0.68 [2.07 – 2.83] | 2.26 ± 0.49 [1.98 – 2.55] | 0.000 | 0.066 | 0.090 |
| Intermediate | 2.34 ± 0.45 [2.10 – 2.57] | 2.27 ± 0.43 [2.03 – 2.52] | 2.60 ± 0.49 [2.32 – 2.87] | 2.195 ± 0.39 [1.96 – 2.42] | ||||
| Final | 2.37 ± 0.47 [2.12 – 2.61] | 2.24 ± 0.39 [2.03 – 2.46] | 2.58 ± 0.56 [2.27 – 2.89] | 2.20 ± 0.50 [1.91 – 2.49] | ||||
| Rectus Femoris Muscle Thickness (cm) | Baseline | 1.63 ± 0.48§ [1.38 – 1.88] | 1.66 ± 0.48 [1.39 – 1.93] | 1.79 ± 0.62 [1.44 – 2.13] | 1.51 ± 0.38 [1.28 – 1.73] | 0.089 | 0.051 | 0.119 |
| Intermediate | 1.84 ± 0.64 [1.51 – 2.17] | 1.71 ± 0.55 [1.40 – 2.01] | 1.72 ± 0.40 [1.50 – 1.95] | 1.52 ± 0.41 [1.27 – 1.76] | ||||
| Final | 1.97 ± 0.56 [1.67 – 2.26] | 1.58 ± 0.59 [1.25 – 1.91] | 1.97 ± 0.60 [1.64 – 2.30] | 1.69 ± 0.43 [1.44 – 1.94] | ||||
| Vastus Lateralis Pennation Angle (°) | Baseline | 12.98 ± 1.89 [12.00 – 13.95] | 12.33 ± 2.37 [11.02 – 13.65] | 13.74 ± 2.63 [12.28 – 15.20] | 12.75 ± 2.90 [11.08 – 14.43] | 0.009 | 0.038 | 0.023 |
| Intermediate | 13.25 ± 3.46 [11.47 – 15.03] | 14.25 ± 3.85 [12.11 – 16.38] | 13.48 ± 3.02 [11.81 – 15.16] | 12.51 ± 3.45 [10.51 – 14.50] | ||||
| Final | 12.95 ± 3.39 [11.20 – 14.69] | 13.61 ± 4.24 [11.26 – 15.97] | 13.63 ± 3.14 [11.89 – 15.37] | 12.58 ± 2.39 [11.19 – 13.96] | ||||
| Rectus Femoris Pennation Angle (°) | Baseline | 9.41 ± 2.64 [8.05 – 10.78] | 8.85 ± 2.57 [7.43 – 10.28] | 9.36 ± 2.46 [7.99 – 10.72] | 9.19 ± 2.16 [7.94 – 10.43] | 0.017 | 0.076 | 0.114 |
| Intermediate | 8.97 ± 2.96 [7.44 – 10.50] | 9.43 ± 3.58 [7.45 – 11.41] | 10.20 ± 2.12 [9.02 – 11.37] | 9.00 ± 2.80 [7.38 – 10.61] | ||||
| Final | 10.70 ± 2.86 [9.22 – 12.17] | 8.49 ± 2.82 [6.93 – 10.06] | 11.37 ± 2.67 [9.89 – 12.86] | 8.28 ± 2.57 [6.80 – 9.77] | ||||
| Vastus Lateralis Fascicle Length (cm) | Baseline | 3.77 ± 1.10 [3.21 – 4.34] | 4.15 ± 1.45 [3.34 – 4.96] | 4.06 ± 1.56 [3.19 – 4.93] | 3.16 ± 0.82 [2.68 – 3.64] | 0.027 | 0.081 | 0.077 |
| Intermediate | 3.51 ± 0.92 [3.03 – 3.98] | 3.22 ± 0.70 [2.83 – 3.60] | 3.60 ± 0.60 [3.26 – 3.93] | 3.67 ± 0.55 [3.34 – 3.99] | ||||
| Final | 3.47 ± 0.78 [3.06 – 3.87] | 3.83 ± 0.64 [3.47 – 4.19] | 3.73 ± 0.59 [3.40 – 4.06] | 3.30 ± 0.74 [2.86 – 3.27] | ||||
| Rectus Femoris Fascicle Length (cm) | Baseline | 2.83 ± 0.50 [2.57 – 3.09] | 2.82 ± 0.71 [2.43 – 3.22] | 2.65 ± 0.62# [2.31 – 3.00] | 3.10 ± 0.65 [2.72 – 3.47] | 0.111 | 0.111 | 0.054 |
| Intermediate | 3.13 ± 0.71 [2.76 – 3.49] | 3.08 ± 0.62 [2.73 – 3.42] | 3.35 ± 0.48 [3.08 – 3.62] | 3.21 ± 0.47 [2.94 – 3.48] | ||||
| Final | 2.97 ± 0.64 [2.64 – 3.30] | 3.25 ± 0.60 [2.92 – 3.59] | 3.16 ± 0.55 [2.85 – 3.47] | 3.58 ± 0.64 [3.21 – 3.95] | ||||
| Single Leg Hop Test (cm) | Baseline | 151.37 ± 29.22# [136.34 – 166.39] | 149.38 ± 26.09# [134.94 – 163.83] | 154.57 ± 35.54# [134.89 – 174.25] | 334.29 ± 55.28# [302.37 – 366.20] | 0.934 | 0.018 | 0.059 |
| Intermediate | 328.47 ± 69.40 [292.79 – 364.15] | 344.53 ± 42.97 [320.74 – 368.33] | 318.40 ± 74.90 [276.92 – 359.88] | 317.36 ± 67.85 [278.18 – 356.53] | ||||
| Final | 330.24 ± 66.59 [296.00 – 364.47] | 354.87 ± 40.63 [332.37 – 377.37] | 331.20 ± 76.58 [288.79 – 373.61] | 334.29 ± 55.28 [302.37 – 366.20] |
Values presented as mean ± SD [95 % confidence interval].
HLET-BFR: high-load eccentric training associated with blood flow restriction; LLET-BFR: low-load eccentric training associated with blood flow restriction; HLET: high-load eccentric training; LLET: low-load eccentric training; Nm: Newton-metre; cm: centimeter; ES¹: intragroup effect size; ES²: intergroup effect size; ES³: effect size on moment vs group interaction.


Regarding eccentric peak torque, statistically significant differences were observed in the group vs. moment interaction (p = 0.002), with a large effect size (ES=0.168). In addition, there was an intergroup difference (p = 0.040) with a moderate effect size (ES=0.135) at the intermediate moment between HLET and LLET in which the high-load group was superior to the low-load group. At the end of training, significant differences were found between LLET and LLET-BFR in relation to HLET, with HLET demonstrating superiority in relation to the other groups. In relation to the intermediate and final moments, statistically significant differences were found in relation to the baseline moment in the HLET-BFR, LLET-BFR, and HLET.
For the isometric and concentric peak torque, no intergroup differences were observed, however differences between moments were identified for the isometric peak torque (p = 0.003 and a moderate effect size=0.097) in the HLET-BFR of the final moment in relation to the baseline moment and in the LLET-BFR of the intermediate moment in relation to the baseline moment. For the concentric peak torque (p < 0.001) significant differences were identified between intermediate and final moments in relation to the baseline, in the HLET-BFR and HLET, with a large effect size (ES=0.245).
In the ultrasound, no statistically significant differences were found for the thickness of the VL muscle at any moments (p = 0.997), moment vs. group interaction (p = 0.091), or groups (p = 0.268). For the RF muscle, there was a significant difference in the moment vs. group interaction (p = 0.023 and moderate effect size=0.119) and the final moment in relation to baseline (p = 0.04 and small effect size=0.01) only for the HLET-BFR. Regarding the pennation angle, no statistically significant differences were found for VL and RF. In the fascicle length of the RF, a difference was found between the intermediate and final moments in relation to the baseline in the HLET group (p = 0.001 and null effect size=0.111) and no difference in the VL muscle (groups: p = 0.202; moments: p = 0.215 and moment vs. group interaction: p = 0.164).
In the Single Leg Hop Test, no differences were found between groups (p = 0.784) and in the moment vs. group interaction (p = 0.317), but differences were found (p < 0.001 and large effect size=0.934) between the intermediate and final moments in relation to baseline in all groups.
DiscussionThe main findings of this study were that for eccentric peak torque in the first three weeks, HLET was superior to LLET, but similar to LLET-BFR. In the last three weeks of training, this superiority was observed in relation to LLET-BFR; however, there was no difference in relation to HLET-BFR. For the outcomes of isometric and concentric peak torque, muscle structure, and performance, there were no differences between groups.
Although there were no statistical differences between the groups, it is clear that there were intragroup differences between the intermediate and baseline moments, with increased eccentric strength in all groups, except for the low-load group without BFR. This result demonstrates that BFR causes an additional effect to eccentric training alone performed at low-load.
In addition, it is worth mentioning that, in order of gains, positive responses from HLET can be observed in the first three weeks, followed by HLET-BFR, and finally LLET-BFR. However, in the final three weeks of training it was observed that the order of gains changed (LLET-BFR, followed by HLET, LLET, and finally HLET-BFR), that is, from the middle to the end of the training the LLET-BFR elicited more positive responses than HLET and HLET-BFR, which had shown more gains in the first three weeks of training. This condition demonstrates that in the case of strength, low-load training associated with BFR is time-dependent,15 i.e., the effect size increases significantly over the weeks of the intervention.
The results also show the greatest increases in strength in eccentric contractions, followed by gains or not in concentric and isometric forces, which corroborates the order of gains in other studies.6,16 Therefore, it seems that the knee extensor muscles adapt more specifically to the type of training performed by the participants, showing that the specificity of the training must also be respected for conditions associated with BFR.
The increases in eccentric strength in the first three weeks in each group, except for LLET, corroborate the result of Baroni et al.6 who reported the time course of neuromuscular adaptations in an eccentric training protocol of 12 weeks with maximum repetitions in the first four weeks of training. This increase in the first three weeks of eccentric training associated or not with BFR can be explained by motor learning related to the eccentric contraction itself.6
Studies show that in eccentric contractions, the proprioceptive feedback of afferent neurons directly influences the performance of eccentric actions,16,17 a fact that promotes greater neural adaptation in the initial training weeks. This aspect is important for clinical applicability, in which the prescription of eccentric training, including associated with BFR, can be used for optimization of time in muscle strength gains.
The increases in isometric strength in the HLET-BFR (after six weeks of training) and LLET-BFR groups (after three weeks of training) and concentric in the HLET-BFR and HLET groups (after three and at the end of six weeks of training, respectively) corroborates the study by Coratella et al.18 in which there was an increase in concentric, eccentric, and isometric peak torque in a group that performed six weeks of eccentric training with maximum contractions of knee extensors in the isokinetic dynamometer.
Regarding isometric peak torque, in the study by Yasuda et al.19 there was also no significant difference in the isometric peak torque in a group that performed eccentric training of 30 % 1RM associated with elbow flexor BFR after a six-week period. On the other hand, Duhig et al.20 found a significant difference in a group that performed eccentric training of knee flexors (Nordic exercise) for five weeks.
Considering the outcome of muscle hypertrophy, the mechanism by which BFR promotes this adaptation remains to be fully elucidated. Regarding the thickness of the VL and RF, no differences were observed between groups and between moments. This result corroborates the study by Timmins et al.21 in which participants performed eccentric training of the knee flexors without BFR in the isokinetic dynamometer, three times a week for six weeks, with maximum contractions. The authors did not observe differences in muscle thickness between moments or compared to the group that performed concentric training.
Yasuda et al.19 compared concentric training with eccentric training in the elbow flexors of young men, both associated with BFR, performed with a load of 30 % 1RM and BFR that reached 160 mmHg The training was performed three times a week for six weeks and demonstrated that the gain in muscle hypertrophy was greater in the concentric group and that in the eccentric group there were no significant changes in volume and cross-sectional area.
The mechanism that involves the change in muscle structure in eccentric exercise is currently under discussion. Some studies22,23 demonstrate that eccentric exercise alone is able to facilitate a change, mainly in the fascicle length, in comparison with conventional resistance training (which includes consecutive phases of eccentric and concentric contractions) and with isolated concentric exercise. This reinforces the concept longitudinal muscle growth is linked to muscle stretching contractions that theoretically imply in the addition of sarcomeres in series.23 However, in the present study, were not found changes in muscle structure
Muscle activations during submaximal training are lower in eccentric contractions compared to concentric contractions.19 Taking into account, that greater muscle activation may be an important factor for muscle hypertrophy,19 the fact that the study performed eccentric actions may have contributed to the findings. In addition, when performing BFR exercises, greater muscle activation occurs in order to compensate for the deficit in the development of secondary strength, through changes in energy supply resulting from reduced oxygen availability to the muscle and greater accumulation of metabolites.24 However, the percentage of BFR used in the present study does not seem to have been sufficient to promote significant changes in muscle structure, despite the fact that studies12 with 40 % of the BFR indicate positive effects on the outcome of muscle strength and thickness with training load of 40 % of 1RM, the exercises performed were classic concentric/eccentric, which differs from this study. Thus, it is hypothesized that the combination of eccentric actions with the low percentage of BFR may explain the lack of differences in hypertrophic responses. Despite this, it should be noted that percentages from 40 to 60 % of BFR during exercise have been recommended for the safety of the method.25
Another issue concerns the location of the ultrasound, as the type of contraction seems to mediate specific hypertrophy of the region, and eccentric training tends to induce greater increases in the size of the muscle in the distal region, while hypertrophy at the middle level of the muscle occurs largely after concentric training.23
Another hypothesis that may explain the findings of muscle hypertrophy is the periodization of the proposed training, which did not aim to reach muscle fatigue, as muscle fatigue is one of the mechanisms proposed in the literature to increase muscle volume,26 or else the performance of maximum contraction during training on the isokinetic dynamometer6,27 or overload training (+100 % maximum voluntary contraction torque).
Gibala et al.28 conducted a study with untrained young men who performed two elbow flexion-training sessions with 80 % of 1RM, one eccentric and the other concentric. The results of muscle biopsies immediately and 48 h after each type of contraction showed, respectively, 82 % and 80 % of muscle fibers injured in eccentric contraction compared with 33 % and 37 % in concentric contraction, demonstrating that the mechanical stress was greater in eccentric exercise. Durand et al.29 measured the lactate accumulation between concentric and eccentric training and observed that concentric exercise promoted more than twice the metabolic stress when compared to eccentric exercise.
Therefore, considering that the mechanical stress caused by eccentric exercise is greater than in concentric contraction, and on the other hand, the metabolic stress that occurs in concentric contraction is greater than in eccentric contraction,23 it seems that the muscle damage caused by mechanical stress in the type of training performed combined with the metabolic stress of the BFR did not generate hypertrophic gains.
Consequently, a possible explanation would be that muscle damage caused by eccentric exercise was greater than the ability to generate an increase in muscle thickness. That is, the muscle damage induced by exercise may have been greater than the capacity for protein synthesis. However, it is noteworthy that recent studies demonstrated that the contribution of muscle protein synthesis and exercise-induced muscle damage is still not well understood in the literature with respect to their real contribution to different long-term hypertrophic adaptations to eccentric and concentric exercise.23
The addition of BFR did not influence performance, verified through the Single Leg Hop Test between groups, however BFR led to significant gains at all times with a large effect size. This result corroborates the study by Santos et al.30 in which participants performed an eccentric training without BFR of knee extensors in the isokinetic dynamometer, twice a week for six weeks, and obtained significant gains at the end of the training period.
Performance in functional tests is maximally improved across similar tasks and can be affected by contraction mode, load, speed, and posture.30 Indeed, distances in the Single Leg Hop Test may have increased due to a greater similarity with the training protocol task.30 Furthermore, gains in muscular strength can directly impact improved performance in this test.30
As limitations of the study, we can mention the absence of the analysis of metabolic stress, muscle damage, and muscle activation, which could bring results that would enrich and deepen the discussion of the present study.
However, it is worth mentioning that this is the first randomized controlled study that performed low and high-load eccentric training associated or not with BFR using the isokinetic dynamometer and the biofeedback line for knee extensors in healthy young people. With respect to the clinical applicability of the study, the eccentric training protocol proposed in the study can be used as a LLET-BFR in patients who are unable to perform high-load work to implement muscle strength and healthy individuals to optimize training periodization can use performance and the same protocol.
In addition, LLET-BFR promoted gains in muscle strength and performance similar to HLET in the first three weeks. Thus, the association of BFR could be an applicable alternative to optimize training time and implement muscle strength in LLET.
As future perspectives, high quality randomized controlled trials in healthy populations are recommended, which include a long-term intervention (in addition to 12 weeks of training), explore different percentages of BFR in this type of training and to see how a study using eccentric overload studies would interact with the BFR.
ConclusionA six-week eccentric training program led to strengthening of knee extensors and improved performance, but without an increased hypertrophic response. As LLET-BFR promotes gains similar to HLET in the first three weeks, it can be used to optimize and implement muscle strength and performance in young men.
The authors declare that they have no conflict of interest.
Trial registration: Clinicaltrials.gov - NCT03601104.

