






As the blood pressure (BP) and heart rate (HR) response during the recovery period can be influenced by size of activated muscle mass, it is possible that this variable also has some distinct effects on post-exercise rate pressure product (RPP). The aim of the present study was to investigate and compare the systolic (SBP) and diastolic blood pressure (DBP), HR, and RPP responses during recovery to resistance exercise with different body regions.
Twelve normotensive young men randomly performed three resistance exercise trials with upper limbs (UL), lower limbs (LL), and whole body (WB), and a control session (CON). All exercise trails included 3 sets of 10 repetitions, with 65% of 1-repetition maximum (1RM) with 2 min rest interval between sets and exercises. SBP, DBP, HR, and RPP were measured before and at each 15 min after exercise until 60 min. Blood lactate (bLAC) was also measured before, and at the 1st minute after the end of exercise. Analysis of variance (ANOVA) and Bonferroni post hoc were used to analyze the data, with a p < .05.
The SBP decrease for 60 min after UL, LL, and WB exercise trials was similar, whereas there was no change in post-exercise DBP after the trials. Significant increases were observed in RPP for 15 min after LL, and 30 min after UL and WB. The blood lactate concentration significantly increased after UL, LL and WB resistance exercise when compared to the rest values, as well as in the CON sessions.
UL, LL and WB resistance exercise lead to post-exercise hypotension, similar in magnitude and duration, and almost produce the same cardiovascular responses, despite different muscle mass involvement.
La presión arterial y la frecuencia cardíaca (FC) durante el período de recuperación pueden estar influenciadas por el tamaño de la masa muscular activa, y es posible que esta variable también tenga algunos efectos diferentes sobre el doble producto en el postejercicio (RPP). El objetivo del presente estudio fue investigar y comparar la presión arterial sistólica (PAS) y la presión arterial diastólica (PAD), la FC y el RPP durante la recuperación de ejercicio de resistencia con distintas regiones del cuerpo.
Doce jóvenes normotensos realizaron al azar 3 ensayos de ejercicio de resistencia con los miembros superiores (MS), los miembros inferiores (MI) y todo el cuerpo (TC), y una sesión de control (CON). Todos los tipos de ejercicio incluyeron 3 series de 10 repeticiones con un 65% de 1RM con 2 min de intervalo de descanso entre series y ejercicios. La PAS, la PAD, la FC, y el RPP se midieron antes y cada 15 min después del ejercicio, hasta 60 min. El lactato sanguíneo (lacS) también se midió antes y en el primer minuto después del ejercicio. Los análisis de varianza (ANOVA) y de Bonferroni post hoc se utilizaron para analizar los datos a p ≤ 0,05.
La PAS disminuyó durante los 60 min postejercicio de MS, MI y TC de manera similar, mientras que después del ejercicio la PAD no mostraba ningún cambio. Se observaron aumentos significativos en RPP durante 15 min después del elercicio de MI y 30 min después del de MS y de TC. La concentración lacS aumentó significativamente después del ejercicio de resistencia de MS, de MI y de TC en comparación con los valores de descanso, así como sesiones CON.
Los diferentes ejercicios de resistencia de MS, MI y TC provocan una hipotensión post ejericio de similar magnitud y duración y casi producen las mismas respuestas cardiovasculares, a pesar de que en ellos participa una masa muscular diferente.
Introduction
Hypertension, a main contributing cause of heart disease, is a major public health problem in the world. Physical activity has been recommended as a non-pharmacological alternative in the prevention and treatment of the arterial hypertension.1 Recently, attention has been paid not only on the cardiovascular benefits of exercise training, but also on the effects of one acute exercise session. After an acute exercise bout, blood pressure (BP) levels are reduced for minutes or hours in relation to pre-exercise levels.2, 3, 4 This phenomenon is called post-exercise hypotension (PEH) and has been widely investigated because of its importance for the prevention and treatment of arterial hypertension.1, 2, 4, 5 PEH has been demonstrated after aerobic exercise1 while controversial results have been observed after resistance exercise. Investigators reported increase,6 decrease7, 8, 9, 10 or no change11, 12 in BP after resistance exercise. Also, there are few studies in the literature regarding to investigation and comparison of the hypotensive effects of resistance exercises performed with upper limbs (UL), lower limbs (LL) and whole body (WB). Most studies on WB resistance exercises used several exercise that each one targeting a specific muscle group, involving UL and LL. In this case, Simão et al.13 verified that a single bout of conventional regimen (6-repetition maximum [6RM]) or circuit (50% of 6RM) resistance exercise produces a significant PEH in normotensive subjects, while others12 observed no change in BP after WB resistance exercise. PEH of systolic blood pressure (SBP) and no change of diastolic blood pressure (DBP) are shown after both UL and LL resistance exercises.14 However, some studies observed PEH of SBP only after LL resistance exercise.15
The possible mechanisms underlying PEH include a reduction of sympathetic nerve activity and decreased vascular responsiveness to α-adrenergic receptor activation, which elicit a sustained reduction of peripheral vascular resistance.16 Taking into account vasorelaxation effects, local substances released by exercising muscles may also be involved in PEH.3 At the same relative exercise intensity, the total active muscle mass and absolute metabolic rate would be greater for WB, LL and UL resistance exercise, respectively. It also follows that while intramuscular concentration of metabolites and ions (e.g., adenosine and K+) would be similar for the three modes of exercise, the absolute production of these vasodilator substances and release into the circulation would be greater with WB resistance exercise. Therefore, it can be expected that WB, LL and UL resistance exercise lead to greater decline in BP, respectively, if PEH is mediated by some peripheral factors.
It has been well established that higher size of exercising muscle mass and higher produced metabolites as a result of rose cellular activity can contribute to stimulate increases in HR during resistance exercise.17 The magnitude of neural and hemodynamic responses during resistance exercise is related to size of activated muscle mass.17 Thus, it is possible that activated muscle mass has also different effects on cardiovascular changes after resistance exercise. In this context, HR and rate pressure product (RPP: an index of myocardial oxygen consumption) are increased after WB resistance exercise7 instead, no change has been observed after LL resistance exercise.18
As BP and HR response during the recovery period can be influenced by size of activated muscle mass, it is possible that this variable also has some distinct effects on post-exercise RPP. Therefore, the aim of the present study was to investigate and compare the SBP, DBP, HR and RPP responses during recovery after UL, LL and WB resistance exercises.
Material and methodsTwelve normotensive sedentary males volunteered to participate in this study. All participants were non-smoker, had no history of cardiovascular disease in themselves and their families, were not taking any medication and not engaged in regular physical activity. Subjects who presented SBP >139 mmHg, DBP >89 mmHg, body mass index >24.9 kg/m2 and fat mass >20% were excluded. Complete advice about possible risks and discomfort was given to the participants, and all of them give their written informed consent to participate. Their physical and cardiovascular characteristics are shown in Table 1.

All procedures were in accordance with the Declaration of Helsinki and the study was approved by the Research Ethics Committee of University of Guilan.
Before initiating the tests, a clinical evaluation and BP, body fat mass, body mass index, weight and height measurements were done. Then, they participated in familiarization sessions and 1RM tests were performed in non-consecutive days. Participants randomly carried out exercises in four non-consecutive days with at least 72 h intervals1: resistance exercise for UL,2 resistance exercise for LL,3 resistance exercise for WB and4 a control session (CON). Pre- and post-exercise values of BP, HR, RPP and blood lactate (bLAC) were measured and analyzed.
All measurements were done at 4:00–6:00 pm to control diurnal variation in BP. Participants had been avoided from consuming alcoholic or caffeinated drinks and performing strenuous physical activity in the previous 48 h, and had been instructed to have their last meal 2 h before the beginning of the experimental sessions. The laboratory had a mean temperature of 22 °C and mean relative air humidity of 50%.
For obtaining subject's resting values of BP and HR, they remained in a seated position for 20 min and BP and HR measured each 5 min from 10th min. It carried out three times after 5 min rest in two separate visits by the same experienced observer. Experimental session was postponed to another day if the pre-exercise BP of volunteers were abnormal (SBP > 139, DBP > 89); otherwise, the subject performed exercises (3 sets, 10 repetitions with a workload corresponding to 65% of 1RM, 2 min rest interval between sets and exercises) with UL (shoulder press, lat pull down, bench press and biceps curl), LL (leg press, knee extension, knee flexion and squat) and/or WB (bench press, leg press, lat pull down, knee flexion). Total time of each session was ∼26 min. After exercise trials, BP and HR measured each 15 min for 60 min during post-exercise recovery (R15, R30, R45, and R60) while participants being rested in a sitting position. HR was monitored using Polar® system (T31, Finland). BP was measured using a standard mercury sphygmomanometer (ALPK2, Japan) in a seated position. First and the fifth phases of Korotkoff sounds were taken as SBP and DBP values, respectively.
RPP (=SBP*HR) was calculated, as a reliable predictor of myocardial oxygen demand.19, 20bLAC were measured before and within the 1st minute after the end of exercise from left hand middle fingertip using an auto blood lactate analyzing system (Lactate Scout, Germany) in following order: fingertip was cleaned and disinfected using distilled water and an alcohol pad. Then, the fingertip punctured with lancet and the first drop of blood cleared and second drop placed in the test strip for analyzing the blood lactate.
Similarly, all measurements were done in CON session whilst subject rested on a comfortable chair for 26 min during the period corresponding to exercise in other trials.
1RM testIn two separate sessions and at least 10 days prior to the experiments, participants underwent 1RM tests for the 8 dynamic resistance exercises with free weights (shoulder press, bench press, biceps curl, squat) or universal weight machine station (leg press, knee extension, knee flexion and lat pull-down). They performed two exercises for UL and two exercises for LL in each session. In this regard, a weight that can be lifted maximally to fatigue after 2–10 repetitions has been used to calculate 1RM according to the Brzycki formula.21 Before the 1RM tests, participants underwent two familiarization sessions and familiar with standard exercise techniques.
Statistical analysisNormality of the data was assessed using Kolmogorov–Smirnov test. This assumption was met for all data, so parametric statistic tests were used. Analysis of variance (ANOVA) with repeated measures (4 sessions * 5 time points) and Bonferroni post hoc tests were used to analyze the data. All data analysis carried out at p ≤ 0.05 level using SPSS v.16 software.
ResultsNo significant differences were observed between experimental sessions in pre-exercise values of SBP, DBP and bLAC. Also these variables did not significantly change during CON session.
Blood lactatebLAC concentration significantly increased after UL, LL and WB resistance exercise in compare to the rest, as well as, CON values (p ≤ 0.05). No significant differences were observed in post-exercise bLAC values between UL, LL and WB trials (Table 2).

SBP significantly declined after UL, LL and WB resistance exercise in compare to the rest values at all time points (p ≤ 0.05). In compare to the control trial, significant decline was observed at R30 in WB and LL resistance exercise and at R45 in WB resistance exercise (p ≤ 0.05) but, we observed no significant differences between experimental trials at any time point, as well as, between post-exercise time points in each one.
DBP presented no change after any trials. DBP at R15, R30, R45 and R60 did not differ from resting values for UL, LL and WB. Also, there was no significant difference between UL, LL, WB and CON in all time points (Figure 1).
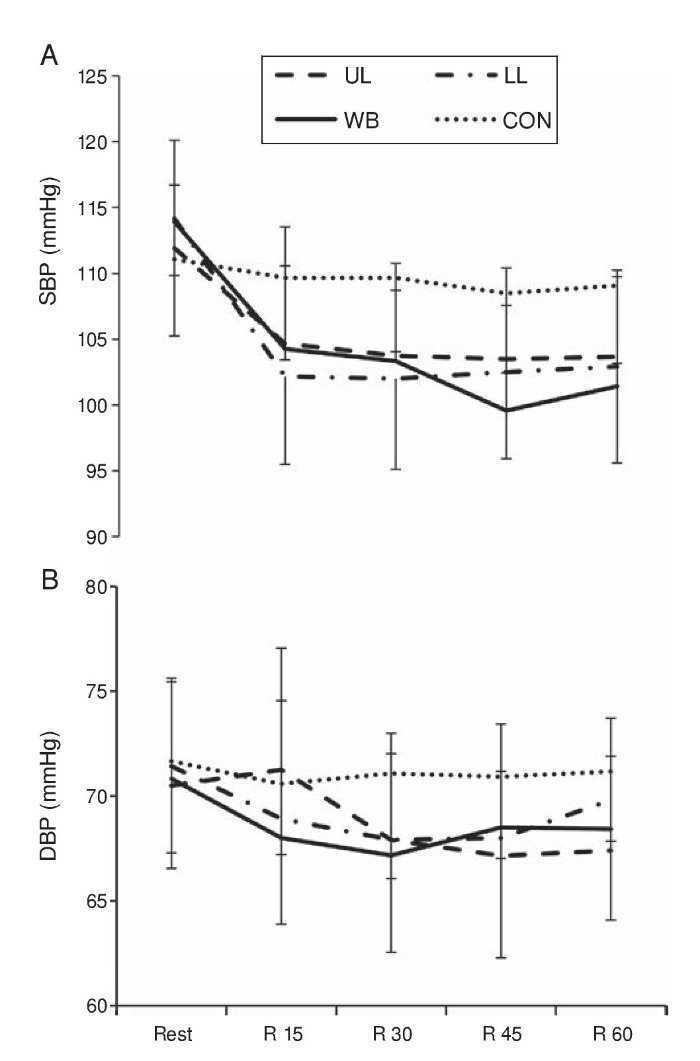
Figure 1. Changes in (A) systolic and (B) diastolic blood pressure during the recovery period.
Heart rateHR remained significantly above rest values after exercise trials (60 min for UL and LL; 45 min for WB; p ≤ 0.05) in compare to the pre-exercise values. In compare to CON trial, HR significantly increased at all time points after UL and WB, and 45 min for LL (p ≤ 0.05). Also, there was no significant difference between UL, LL and WB (Figure 2A).
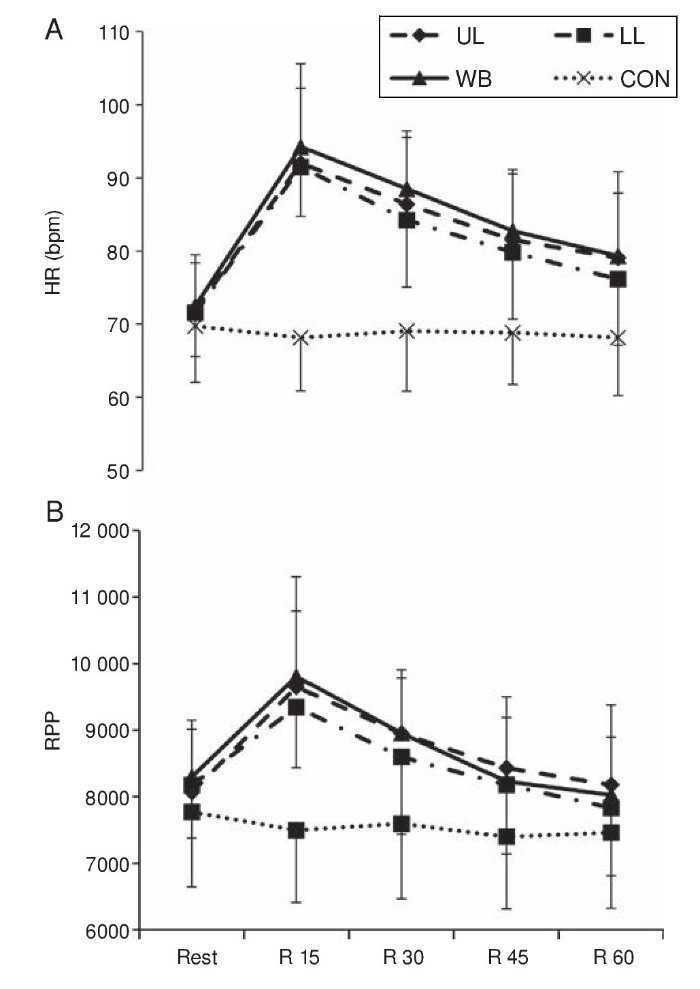
Figure 2. Changes in (A) heart rate and (B) rate pressure product during the recovery period.
RPP significantly increased and remained higher than pre-exercise values, as well as, CON trial, after exercise trials (15 min for LL; 30 min for UL and WB; p ≤ 0.05). Also, there was no significant difference between UL, LL and WB (Figure 2B).
DiscussionBased on previous studies, the data about PEH and resistance exercise, particularly, with UL and LL is still scarce and most studies that have used WB resistance exercise, reported increase,6 decrease7, 8, 9, 10 or no change11, 12 in post-resistance exercise BP. Mohebbi et al. and Rezk et al. observed a decline in the SBP after WB resistance exercise (used some exercises, but each one targeting a specific muscle group, involving upper and lower limbs).7, 8 Dias et al. reported PEH of SBP and no change of DBP followed by both UL and LL resistance exercises and observed no differences for SBP and DBP between the exercise modes.14 In another study, Polito and Farinatti investigated the effects of muscle mass on PEH following resistance exercises (biceps curl vs. leg extension) with 10 repetitions at 12RM workload. They observed PEH of SBP just for the situation that large muscle mass (leg extension) exercised with high volume (10 sets).15 Hence, it is feasible to think that muscle mass and exercise volume, both, can influence the PEH. Furthermore, MacDonald et al. reported PEH of SBP up to 60 min, after 15 min lower limb resistance exercise (leg press) performed with load corresponding to 65% of 1RM.22 In contrast, others23 observed no significant changes in the SBP and DBP after both of traditional multiple set and tri-set methods that six UL exercises were used for two distinct muscular groups (chest and back). Also, no hypotensive response in SBP nor DBP is reported following three sets of 12 maximal repetitions of knee extension unilaterally and bilaterally.18 However, in the present study, the UL, LL and WB resistance exercise performed at 65% of 1RM provoked PEH of SBP during the recovery period, similarly.
In contrast to the results of our study, some studies15, 18, 23 failed to observe significant PEH following UL and/or LL resistance exercise. These conflicting results regarding to recovery blood pressure may be related to involved muscle mass in each exercise. Our subjects performed 3 sets of 10 repetitions of the 4 exercises for UL, LL and WB, that exercising muscle mass were more than in inconsistent studies.15, 23, 24 One of the physiological mechanisms that could explain the influence of muscle mass on blood pressure after resistance exercise is the reduction in vascular resistance, caused by the release of vasodilating endothelial substances (e.g., nitric oxide and prostaglandins). An increase in blood flow seems to be the stimulus for the release of such substances.5 Therefore, it may be assumed that a larger muscle mass activated during the exercise, if all the other variables are kept constant, would raise the need for blood in the active region thus favoring PEH. Moreover, our results showed that UL, LL and WB resistance exercise lead to occurrence of PEH similarly in magnitude and duration after resistance exercise, despite different muscle mass is involved. Although in this study the potential causes of PEH wasn’t measured, but it doesn’t seem that size of activated muscle mass and metabolites produced from cellular activity to be the main cause of PEH. Accordingly, we suggest that the magnitude of muscle mass that is involved in UL exercise is great enough to incidence of post-resistance exercise hypotension.
Resistance exercise protocols typically differ among studies, and these differences may likely be responsible for some of the variations that seen in the results. The exercise intensity, number of sets, rest intervals and stations of resistance exercise in the current study differed from that in inconsistent studies.15, 18, 23 Various degree of produced metabolic stress by these different protocols may be enough to affect recovery blood pressure.
Previous studies on young normotensive humans have shown controversial results in regard to HR behavior during post-exercise period.8, 11, 18, 23 We found that HR increases by exercise and remains significantly higher than rest values after exercise in all experimental trials regardless of size of involved muscles. Increase in HR has also been reported by other studies.7, 8, 23 As same as Rodriguez et al.23 that observed significant increase in HR for 60 min after UL resistance exercise, others7 reported similar increase in HR after whole body resistance exercise that greater muscle mass is involved. However, Polito et al.18 observed no change of HR following three sets of 12 maximal repetitions of knee extension unilaterally and bilaterally. This contradiction is probably due to the use of low number of exercises and sets. Collectively, it does not seem that size of activated muscle mass and produced metabolites from cellular activity to be the main cause of increase in HR. Hence, increased HR after resistance exercise may be mediated by an increase in sympathetic and a decrease in parasympathetic modulation of the heart.8 These autonomic responses might be mediated by baroreflex control evoked by BP decrease16 that we observed after exercise.
The concept that the product of systolic BP and HR (i.e., RPP) is well correlated to myocardium oxygen consumption in young healthy and cardiac patients has been well established.19, 25 We demonstrated that RPP increase after exercise trials and returned to the pre-exercise level 15 min after LL and 30 min after UL and WB. In this context, it has been suggested that HR is the most important factor to determine RPP,17 as confirmed by our results that found a consistency between RPP and HR changes at all time points after exercise.
The results of the bLAC response suggest a same metabolic stress for UL, LL and WB resistance exercise. A significant correlation between bLAC after resistance exercise and BP decrease during post-exercise recovery has been shown by Crisafulli et al. and Moreno et al.26, 27 Therefore, the metabolic stress of resistance exercise (i.e., blood lactate) may have a relation to BP reduction. Lactic acid dissociates to H+ ions and these ions may activate ATP-sensitive K+ (KATP) channels present in vascular smooth muscle. The activation of these channels may lead to smooth muscle hyperpolarization and, consequently, to vascular relaxation and a decrease in BP.26, 27
In conclusion, we showed that the UL, LL and WB resistance exercise elicited PEH of SBP, no change of DBP, increase in HR and RPP in young healthy individuals. SBP declines after UL, LL and WB resistance exercises lasted for at least 60 min, regardless from involved muscle mass. It seems that the magnitude of muscle mass that is involved in UL exercise is great enough to incidence of post-resistance exercise hypotension. However, because resistance exercise allows great manipulation of volume and intensity, the possible interaction between the number of sets and repetitions, number and type of exercises, workload and recovery intervals to produce PEH should be considered in future researches.
We suggest that these exercise modes as a non-pharmaceutical treatment may be helpful in the control of hypertension. We also suggest that UL and LL resistance exercise can be useful for individuals who may have trouble exercising with the upper or lower limbs, such as the handicapped or those who have spinal cord injuries or diabetic foot, besides contributing to the health of those who have an elevated SBP.
Conflict of interestAuthors declare that they do not have any conflict of interests.
Received 3 February 2016
Accepted 2 May 2016
Corresponding author. mohebbi_h@yahoo.com

