





Statements
- •
That it is an original work.
- •
That it has not been previously published in whole or in part.
- •
That it is not under evaluation in any other publication.
- •
That all authors are responsible for the final version of this article, to the preparation of which they have contributed.
- •
That the fact of being accepted for publication implies that all authorship rights are transferred.
- •
That there was not and will not be any economic benefit for the preparation of this manuscript.
- •
That there was no source of funding for the development of the manuscript.
- •
That there are no conflicts of interest.
As a team sport, soccer has undergone a significant evolution over the years, becoming a global phenomenon that attracts passionate crowds.1 In this sport, soccer players must possess a wide range of physical skills, ranging from the ability to make quick changes of direction to explosive jumps, repeated sprints and remarkable endurance, among other skills. Improving these aspects is crucial to enhance in-game performance.2 Nevertheless, due to the intense physical demands of both training and competitive matches, injuries are a recurring problem among soccer players.3
In order to address this problem, numerous studies have been carried out to identify the role of various preventive programs in reducing injuries in soccer players.4-6 One of the most remarkable is FIFA 11+, introduced in 2009 and designed to reduce the risk of musculoskeletal injuries in soccer players. This program was developed by the Fédération Internationale de Football Association (FIFA) in collaboration with international sports medicine experts.7
In addition to the players, it is essential to consider the refereeing corps, whose role is vital for the proper development of this sporting spectacle. Referees, as well as the players, must possess exceptional physical qualities, as they are also subjected to considerable physical exertion. In fact, it has been shown that referees can cover distances of up to 12 kms and run at speeds above 18 kms per hour.8 Therefore, it is not surprising that they also suffer a high number of injuries, mainly in the lower limbs.9 To address this concern, an injury prevention manual specifically designed for referees, known as FIFA 11+ referees, has been proposed.10
However, to date, there is a notable imbalance in the existing literature on injuries between soccer players and soccer referees. Most research efforts have focused primarily on the players, leaving the refereeing corps in the background. This aspect is not only evident in studies evaluating the effectiveness of various preventive programs, including FIFA 11+ in soccer players,4-6 but also in studies that aim to provide epidemiological profiles of injuries based on systematic reviews that allow the inclusion of a larger number of subjects.11 At this time and to the best of our knowledge, there is no work that aims to map existing studies on injury epidemiology in soccer referees to broadly characterize the epidemiological profile of this population with a large number of subjects. Consequently, the aim of this review is to provide a broader epidemiological profile of injuries in male soccer referees by systematically searching for observational scientific studies. In addition, as a secondary outcome, we aim to identify the differences between main and assistant soccer referees in terms of their injury incidence and prevalence.
MethodsStudy designThe present work consists of a systematic review of observational studies, including prospective, retrospective and cross-sectional investigations. For this purpose, the recommendations of the PRISMA (Preferred Reporting Items for Systematic reviews and Meta-Analyses) standards were followed.12 This approach attempted to provide a complete epidemiological profile of injuries in soccer referees, based on the analysis of a large number of subjects. The use of this strategy was justified considering that existing primary studies tend to have relatively small samples. Thus, conducting a review covering a larger number of subjects allowed to obtain a broader and more representative view of the situation. Furthermore, to date there is no knowledge of the existence of such a review, which underscores the relevance and originality of this study. This review, following its prior registration in PROSPERO, has been assigned the number CRD42024547881.
Criteria for the assessment of studies for this reviewTypes of studiesFor this review, observational studies of various types were considered, including prospective, retrospective and cross-sectional studies, without language restrictions, that provided relevant information on the epidemiology of injuries in both main and assistant soccer referees.
Type of target study populationGiven that the anatomical, genetic and hormonal differences between women and men can drastically influence the prevalence and incidence of injuries, the scope of this review was limited to male soccer referees. Studies reporting injuries occurring in male main referees and assistant referees, discriminated by anatomic location or diagnosis, were included for the purpose of designing an epidemiologic profile of injuries in this population. Additionally, studies in which the population was recruited based on a pre-existing pathology were excluded, as well as those in which referees participated in beach soccer, indoor soccer or other variants, maintaining the specific focus on 11-a-side soccer referees, given that injuries may vary according to the environment in which they perform.
Types of outcome measureThe outcomes sought in the studies included reporting the number of injuries occurring in male soccer referees, both main and assistant referees, during any given time period. Two conditions were set for the inclusion of studies: first, the injury report was required to discriminate injuries by anatomical location or diagnosis, excluding those studies that provided overall injury reports without specifying a particular profile. Second, injury reporting was required to distinguish between main and assistant referees, as physical and mental demands may vary considerably depending on the specific role within the refereeing.
Search strategy and procedureA systematic search of observational studies with a cut-off date of May 24, 2024, was conducted using the databases PubMed, Web of Science and ScienceDirect. For this purpose, the following search terms were used: Epidemiology, Epidemiologic, Epidemiological, Incidence, Prevalence, Injury, Injuries, Injured, Soccer and Soccer referees. These terms were combined in the following search equation: ((((((Epidemiology) OR (Epidemiologic)) OR (Epidemiological)) OR (Incidence)) OR (Prevalence)) AND (((Injury) OR (Injuries)) OR (Injured))) AND (("Soccer referees") OR (Soccer)). In the complementary material, the search history in each of the databases used, together with the number of records identified, is provided in detail.
Identification of studies and data extractionThe text selection process for this review was carried out in a rigorous and systematic manner. First, preliminary manuscripts obtained during the searches in each database were uploaded to the collaborative web application Rayyan.13 Then, two reviewers carried out an independent selection after analyzing the title and abstract of each text found. Subsequently, the reviewers carried out a second independent selection process after reading the full texts that had been selected in the first phase. During these two stages of selection, in the event of discrepancies between the reviewers, a third reviewer was involved to facilitate reaching a consensus and reaching an agreement.
Once the texts included in this review had been selected, the following data were extracted from each of them: title, authors, year of publication, journal of publication, type of study, follow-up period, injury definition, population, total number of injuries, and number of injuries by anatomic location or diagnosis, as applicable. These data were extracted by two reviewers independently and stored in an Excel spreadsheet. Subsequently, the extracted data were cross-checked to verify the accuracy of the extraction. In case of discrepancies, a third reviewer intervened to verify the information and reach a consensus on the final data.
Quality of the studiesThe quality of the manuscripts included in this review was assessed using the STROBE checklist,14 which provides predefined criteria to classify the quality of manuscripts according to their presentation and reporting. It is important to note that STROBE does not constitute a quality scale of the evidence itself, but rather focuses on the quality of the study report. Therefore, to complement the assessment of study quality, we used the checklist for cohort studies provided by SIGN (Scottish Intercollegiate Guidelines Network) .15 This list contributed to the evaluation of the quality and methodological rigor of each of the selected studies. The application of these scales to the selected texts in this review was carried out by two investigators. In case of disagreements, a third reviewer intervened to facilitate consensus.
Analysis and synthesis of resultsThe results obtained in this study are presented quantitatively using descriptive statistics through tables and figures, which provide a visual representation of the data collected. These tables and figures show the prevalence and incidence of injuries in soccer referees, discriminated by anatomical location or specific diagnosis, as applicable. In addition, the results are presented qualitatively through a narrative that describes and analyzes the findings obtained. This qualitative narrative provides a detailed interpretation of the results, highlighting trends and patterns observed in the data.
To obtain the prevalence of injuries, retrospective and cross-sectional studies were used, while prospective studies were used exclusively to obtain the incidence of injuries. As previously mentioned, data were collected on the location and diagnosis of injuries, which were subsequently analyzed and operationalized according to the temporal period of analysis to obtain measures of prevalence and incidence. The ratio of injury incidence and prevalence data was calculated by dividing the total number of injuries per anatomic region or specific pathology by the total number of injuries reported in all anatomic locations or pathologies, respectively.
ResultsCharacteristics of the study selectionIn the systematic search, 12,246 manuscripts were identified, of which 2460 were from PubMed, 2790 from Web of Science, and 6996 from ScienceDirect. This was reduced to 10,479 after eliminating duplicates. Once the titles and abstracts had been reviewed, 12 articles were selected for full review.9,16-26 Following this review, 6 articles presenting combined data for main and assistant referees were excluded,16,18-22 and one more, since it did not provide specific data for soccer referees,17 leaving a total of 5 articles for the final selection and synthesis.9,23-26Fig. 1 provides the flow chart summarizing the search and item selection process.

PRISMA flow chart suggested by Page et al.27
An analysis was carried out covering a total of 433 main referees and 467 assistant referees. Of these, 763 were examined to determine the prevalence of injuries, distributed in 382 main referees and 381 assistant referees, while 137 were studied to analyze the incidence of injuries, of which 51 were main referees and 86 were assistant referees. The age of the referees ranged from 25 to 45 years old.
In terms of the methodology used, three retrospective studies were identified that contributed to the prevalence analysis [9, 25 y 26], a prospective study used for incidence analysis,23 and another study that presented both prospective and retrospective characteristics, thus allowing the analysis of both the incidence and prevalence of injuries.24
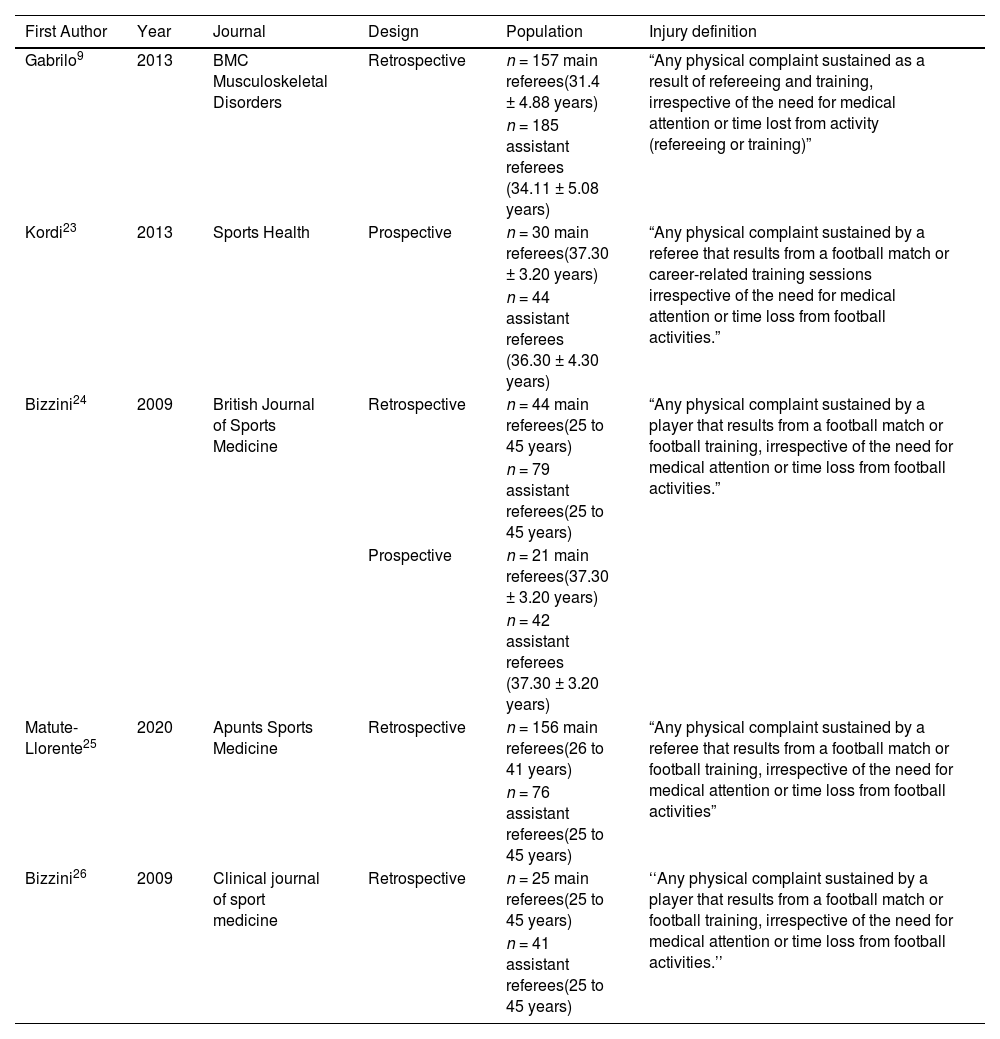
A noteworthy aspect of this analysis was the consistency in the definition of injury used among the studies. Although some of them adopted literal definitions previously used in research on soccer players, others made slight adaptations, replacing terms such as "soccer players" or "footballers" with "referees". However, all studies agreed to consider an injury as any physical ailment resulting from soccer matches or training sessions related to refereeing, regardless of the need for medical attention or interruption of soccer activities. For a more detailed understanding of the characteristics of the included studies, a summary is presented in Table 1.
Characteristics of the included studies.
| First Author | Year | Journal | Design | Population | Injury definition |
|---|---|---|---|---|---|
| Gabrilo9 | 2013 | BMC Musculoskeletal Disorders | Retrospective | n = 157 main referees(31.4 ± 4.88 years) | “Any physical complaint sustained as a result of refereeing and training, irrespective of the need for medical attention or time lost from activity (refereeing or training)” |
| n = 185 assistant referees (34.11 ± 5.08 years) | |||||
| Kordi23 | 2013 | Sports Health | Prospective | n = 30 main referees(37.30 ± 3.20 years) | “Any physical complaint sustained by a referee that results from a football match or career-related training sessions irrespective of the need for medical attention or time loss from football activities.” |
| n = 44 assistant referees (36.30 ± 4.30 years) | |||||
| Bizzini24 | 2009 | British Journal of Sports Medicine | Retrospective | n = 44 main referees(25 to 45 years) | “Any physical complaint sustained by a player that results from a football match or football training, irrespective of the need for medical attention or time loss from football activities.” |
| n = 79 assistant referees(25 to 45 years) | |||||
| Prospective | n = 21 main referees(37.30 ± 3.20 years) | ||||
| n = 42 assistant referees (37.30 ± 3.20 years) | |||||
| Matute-Llorente25 | 2020 | Apunts Sports Medicine | Retrospective | n = 156 main referees(26 to 41 years) | “Any physical complaint sustained by a referee that results from a football match or football training, irrespective of the need for medical attention or time loss from football activities” |
| n = 76 assistant referees(25 to 45 years) | |||||
| Bizzini26 | 2009 | Clinical journal of sport medicine | Retrospective | n = 25 main referees(25 to 45 years) | ‘‘Any physical complaint sustained by a player that results from a football match or football training, irrespective of the need for medical attention or time loss from football activities.’’ |
| n = 41 assistant referees(25 to 45 years) |
Note: The referees are professional.
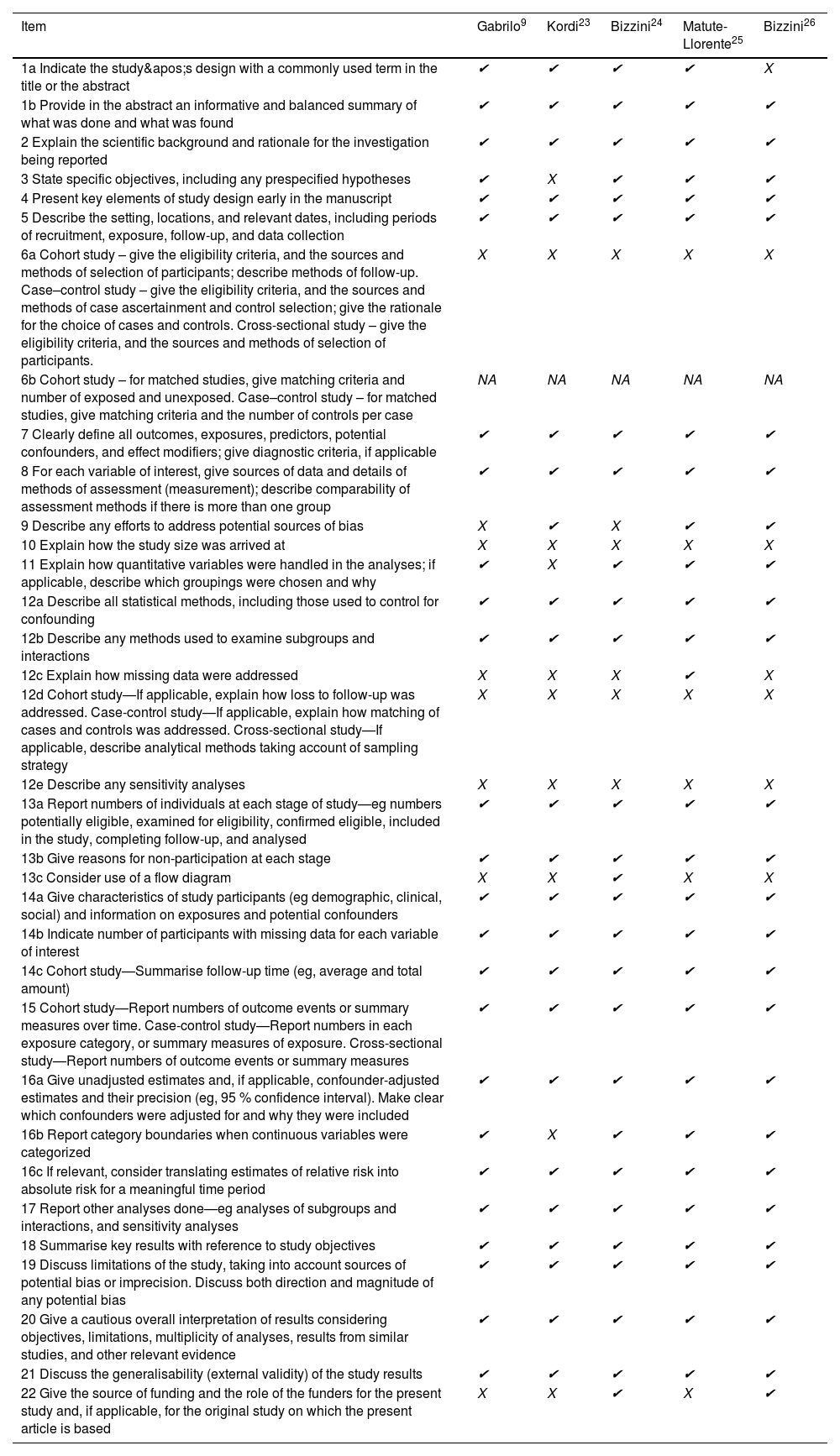
After performing an assessment of the degree of compliance of each study's report using the STROBE list, it was observed that the main weakness among the articles reviewed was related to several aspects. These included population eligibility criteria, sample size calculation, handling of missing data, dealing with loss to follow-up, sensitivity analysis, and notably, the limited use of flowcharts to facilitate understanding of the flow of subjects throughout the study, except for one study that employed this tool.
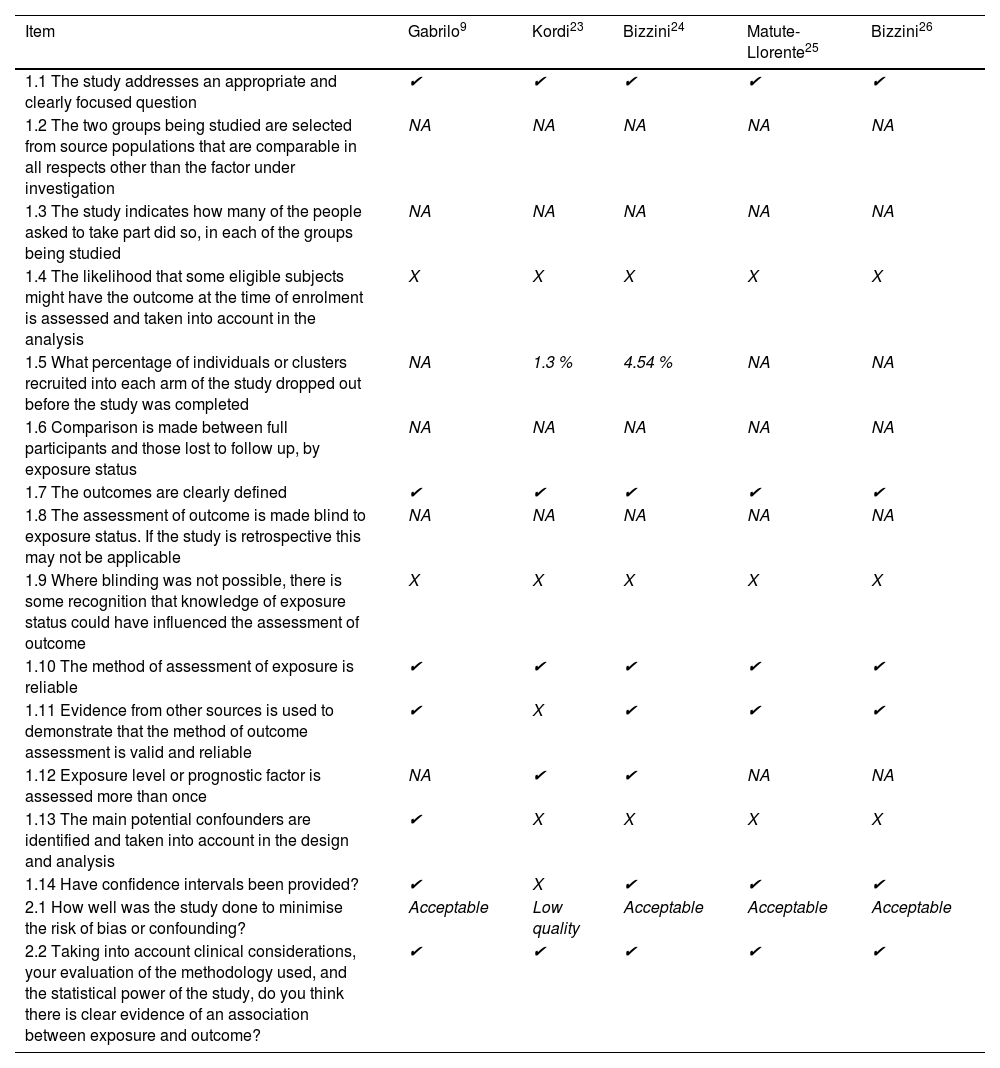
Regarding quality assessment, upon completion of the cohort study checklist provided by SIGN, one study was identified as being of low quality, while four of them were considered to be of acceptable quality. Among the aspects that presented major deficiencies were the assessment of the probability that some eligible subjects may present the outcome of interest at enrollment, the blinding or lack of recognition of blinding in those cases where it was impossible, and the identification and control of potential confounders. A summary of the reporting grade and quality of the studies included in this review is provided in Tables 2 and 3.
Assessment of study reports using STROBE.
| Item | Gabrilo9 | Kordi23 | Bizzini24 | Matute-Llorente25 | Bizzini26 |
|---|---|---|---|---|---|
| 1a Indicate the study's design with a commonly used term in the title or the abstract | ✔ | ✔ | ✔ | ✔ | X |
| 1b Provide in the abstract an informative and balanced summary of what was done and what was found | ✔ | ✔ | ✔ | ✔ | ✔ |
| 2 Explain the scientific background and rationale for the investigation being reported | ✔ | ✔ | ✔ | ✔ | ✔ |
| 3 State specific objectives, including any prespecified hypotheses | ✔ | X | ✔ | ✔ | ✔ |
| 4 Present key elements of study design early in the manuscript | ✔ | ✔ | ✔ | ✔ | ✔ |
| 5 Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data collection | ✔ | ✔ | ✔ | ✔ | ✔ |
| 6a Cohort study – give the eligibility criteria, and the sources and methods of selection of participants; describe methods of follow-up. Case–control study – give the eligibility criteria, and the sources and methods of case ascertainment and control selection; give the rationale for the choice of cases and controls. Cross-sectional study – give the eligibility criteria, and the sources and methods of selection of participants. | X | X | X | X | X |
| 6b Cohort study – for matched studies, give matching criteria and number of exposed and unexposed. Case–control study – for matched studies, give matching criteria and the number of controls per case | NA | NA | NA | NA | NA |
| 7 Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers; give diagnostic criteria, if applicable | ✔ | ✔ | ✔ | ✔ | ✔ |
| 8 For each variable of interest, give sources of data and details of methods of assessment (measurement); describe comparability of assessment methods if there is more than one group | ✔ | ✔ | ✔ | ✔ | ✔ |
| 9 Describe any efforts to address potential sources of bias | X | ✔ | X | ✔ | ✔ |
| 10 Explain how the study size was arrived at | X | X | X | X | X |
| 11 Explain how quantitative variables were handled in the analyses; if applicable, describe which groupings were chosen and why | ✔ | X | ✔ | ✔ | ✔ |
| 12a Describe all statistical methods, including those used to control for confounding | ✔ | ✔ | ✔ | ✔ | ✔ |
| 12b Describe any methods used to examine subgroups and interactions | ✔ | ✔ | ✔ | ✔ | ✔ |
| 12c Explain how missing data were addressed | X | X | X | ✔ | X |
| 12d Cohort study—If applicable, explain how loss to follow-up was addressed. Case-control study—If applicable, explain how matching of cases and controls was addressed. Cross-sectional study—If applicable, describe analytical methods taking account of sampling strategy | X | X | X | X | X |
| 12e Describe any sensitivity analyses | X | X | X | X | X |
| 13a Report numbers of individuals at each stage of study—eg numbers potentially eligible, examined for eligibility, confirmed eligible, included in the study, completing follow-up, and analysed | ✔ | ✔ | ✔ | ✔ | ✔ |
| 13b Give reasons for non-participation at each stage | ✔ | ✔ | ✔ | ✔ | ✔ |
| 13c Consider use of a flow diagram | X | X | ✔ | X | X |
| 14a Give characteristics of study participants (eg demographic, clinical, social) and information on exposures and potential confounders | ✔ | ✔ | ✔ | ✔ | ✔ |
| 14b Indicate number of participants with missing data for each variable of interest | ✔ | ✔ | ✔ | ✔ | ✔ |
| 14c Cohort study—Summarise follow-up time (eg, average and total amount) | ✔ | ✔ | ✔ | ✔ | ✔ |
| 15 Cohort study—Report numbers of outcome events or summary measures over time. Case-control study—Report numbers in each exposure category, or summary measures of exposure. Cross-sectional study—Report numbers of outcome events or summary measures | ✔ | ✔ | ✔ | ✔ | ✔ |
| 16a Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (eg, 95 % confidence interval). Make clear which confounders were adjusted for and why they were included | ✔ | ✔ | ✔ | ✔ | ✔ |
| 16b Report category boundaries when continuous variables were categorized | ✔ | X | ✔ | ✔ | ✔ |
| 16c If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period | ✔ | ✔ | ✔ | ✔ | ✔ |
| 17 Report other analyses done—eg analyses of subgroups and interactions, and sensitivity analyses | ✔ | ✔ | ✔ | ✔ | ✔ |
| 18 Summarise key results with reference to study objectives | ✔ | ✔ | ✔ | ✔ | ✔ |
| 19 Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and magnitude of any potential bias | ✔ | ✔ | ✔ | ✔ | ✔ |
| 20 Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from similar studies, and other relevant evidence | ✔ | ✔ | ✔ | ✔ | ✔ |
| 21 Discuss the generalisability (external validity) of the study results | ✔ | ✔ | ✔ | ✔ | ✔ |
| 22 Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on which the present article is based | X | X | ✔ | X | ✔ |
Note= ✔: Yes; X: No; NA: Not applies.
Assessment of the quality of the studies using SIGN.
| Item | Gabrilo9 | Kordi23 | Bizzini24 | Matute-Llorente25 | Bizzini26 |
|---|---|---|---|---|---|
| 1.1 The study addresses an appropriate and clearly focused question | ✔ | ✔ | ✔ | ✔ | ✔ |
| 1.2 The two groups being studied are selected from source populations that are comparable in all respects other than the factor under investigation | NA | NA | NA | NA | NA |
| 1.3 The study indicates how many of the people asked to take part did so, in each of the groups being studied | NA | NA | NA | NA | NA |
| 1.4 The likelihood that some eligible subjects might have the outcome at the time of enrolment is assessed and taken into account in the analysis | X | X | X | X | X |
| 1.5 What percentage of individuals or clusters recruited into each arm of the study dropped out before the study was completed | NA | 1.3 % | 4.54 % | NA | NA |
| 1.6 Comparison is made between full participants and those lost to follow up, by exposure status | NA | NA | NA | NA | NA |
| 1.7 The outcomes are clearly defined | ✔ | ✔ | ✔ | ✔ | ✔ |
| 1.8 The assessment of outcome is made blind to exposure status. If the study is retrospective this may not be applicable | NA | NA | NA | NA | NA |
| 1.9 Where blinding was not possible, there is some recognition that knowledge of exposure status could have influenced the assessment of outcome | X | X | X | X | X |
| 1.10 The method of assessment of exposure is reliable | ✔ | ✔ | ✔ | ✔ | ✔ |
| 1.11 Evidence from other sources is used to demonstrate that the method of outcome assessment is valid and reliable | ✔ | X | ✔ | ✔ | ✔ |
| 1.12 Exposure level or prognostic factor is assessed more than once | NA | ✔ | ✔ | NA | NA |
| 1.13 The main potential confounders are identified and taken into account in the design and analysis | ✔ | X | X | X | X |
| 1.14 Have confidence intervals been provided? | ✔ | X | ✔ | ✔ | ✔ |
| 2.1 How well was the study done to minimise the risk of bias or confounding? | Acceptable | Low quality | Acceptable | Acceptable | Acceptable |
| 2.2 Taking into account clinical considerations, your evaluation of the methodology used, and the statistical power of the study, do you think there is clear evidence of an association between exposure and outcome? | ✔ | ✔ | ✔ | ✔ | ✔ |
Note= ✔: Yes; X: No; ?: Can't say; NA: Not applies. The percentages shown in item 1.5 correspond to the average number of subjects who dropped out of the study before its completion.
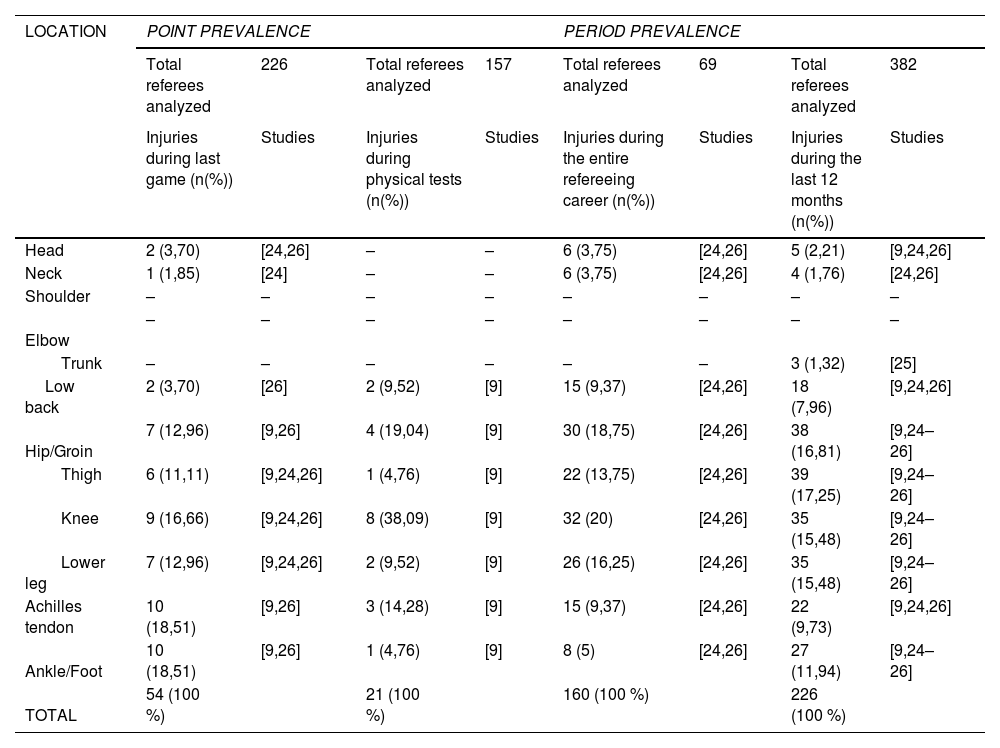
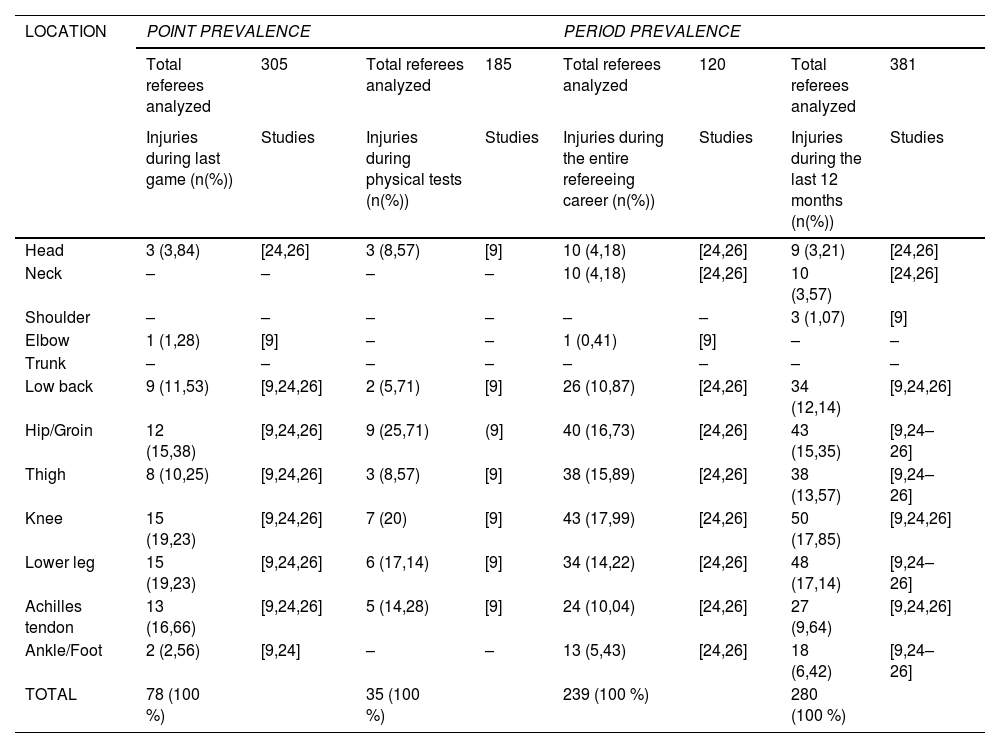
The most prevalent injury by anatomical location for main referees, according to the last match, was injuries in the Achilles tendon and ankle/foot, while for assistant referees was in the lower leg. During the physical tests, the most common injuries for the main referees were in the knee, hip and groin, and in the hip and groin for the assistant referees. Throughout their career, the most common injuries were in the hip and groin for the main referees, and in the knee for the assistant referees. In the last twelve months, the most common injury was in the thigh for main referees, and again in the knee for assistant referees. Table 4 provides a detailed summary of the prevalence of injuries, categorized by anatomical location, for the main referees. Similarly, Table 5 presents this information for the assistant referees.
Prevalence of injuries in main referees categorized by different anatomical locations.
Prevalence of injuries in assistant referees categorized by different anatomical locations.
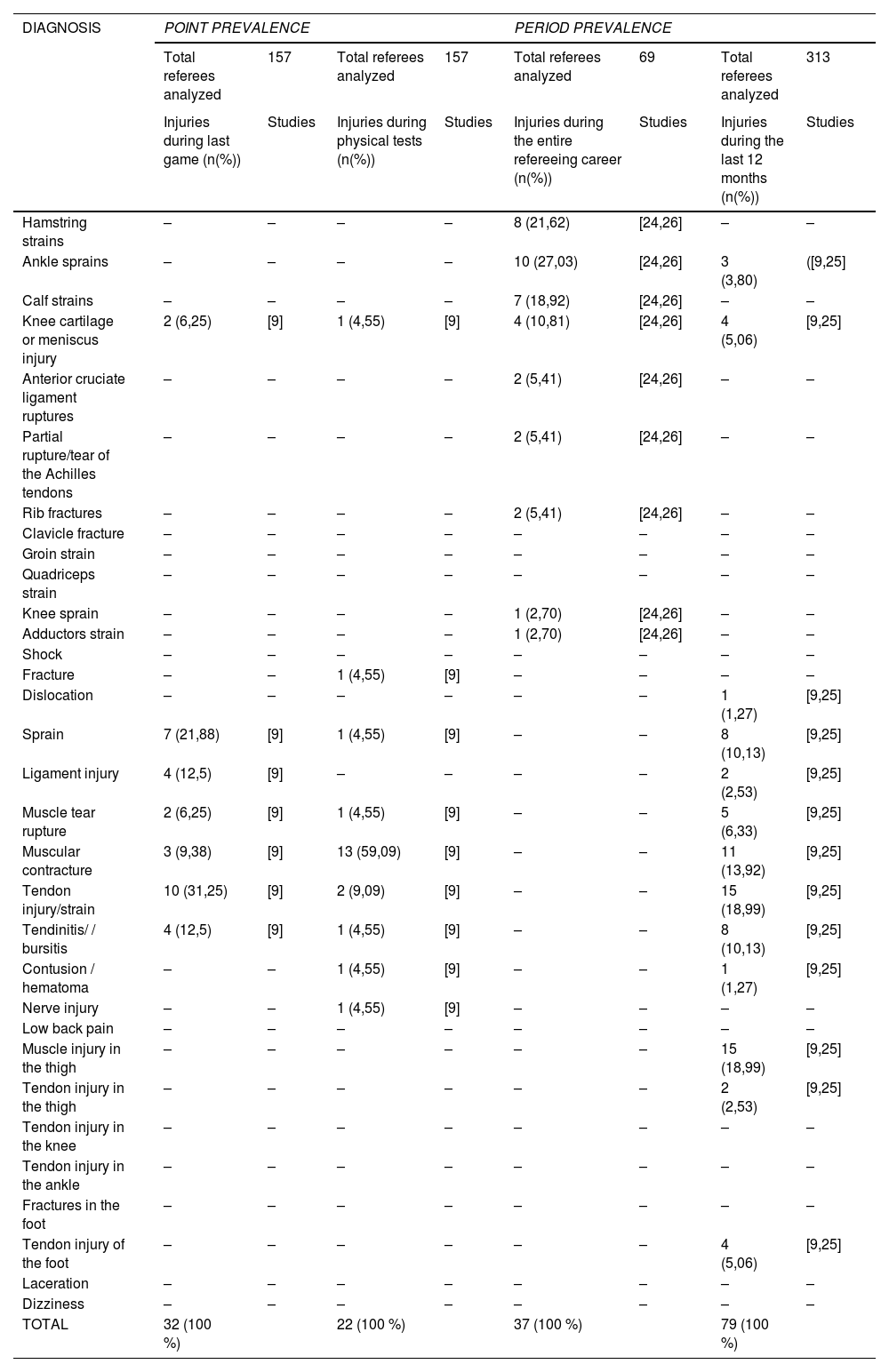
On the other hand, in the last match mediated by the main referees, tendon strain was identified as the most prevalent diagnosis, while during the physical tests, "muscle contracture" was the most reported. Throughout their careers as referees, ankle sprains were the most prevalent diagnosis. Finally, during a 12-month follow-up, thigh muscle injuries and tendon strains again stood out as the most prevalent.
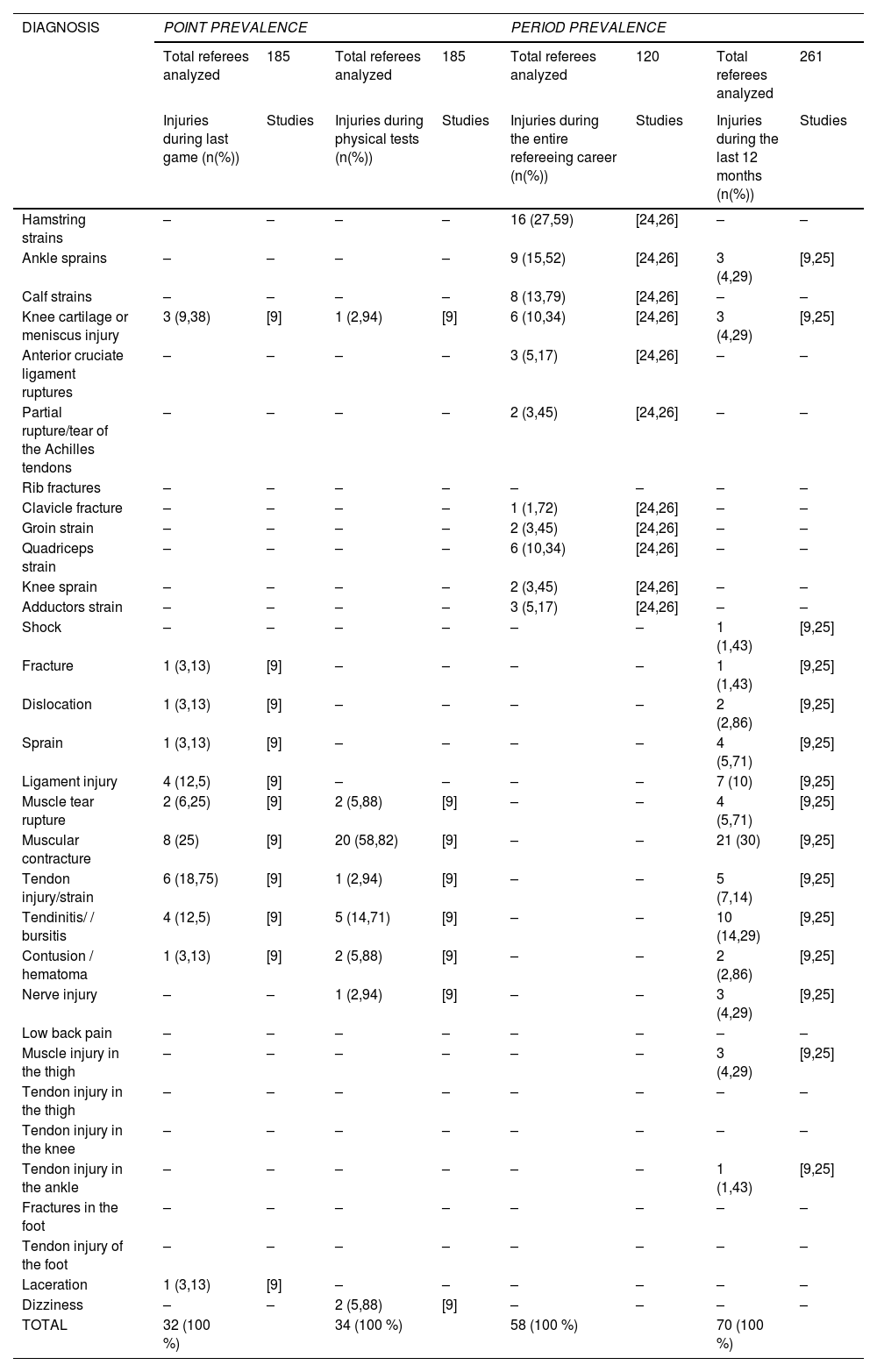
In the case of assistant referees, "muscle contracture" emerged as the most common diagnosis both in the last match refereed and during physical tests and 12-month follow-up. On the other hand, hamstring strains were established as the most prevalent throughout their career. An exhaustive analysis of the prevalence of injuries discriminated by diagnosis for main and assistant referees is detailed in Tables 6 and 7 respectively.
Prevalence of injuries in main referees categorized by diagnosis.
Prevalence of injuries in assistant referees categorized by diagnosis.
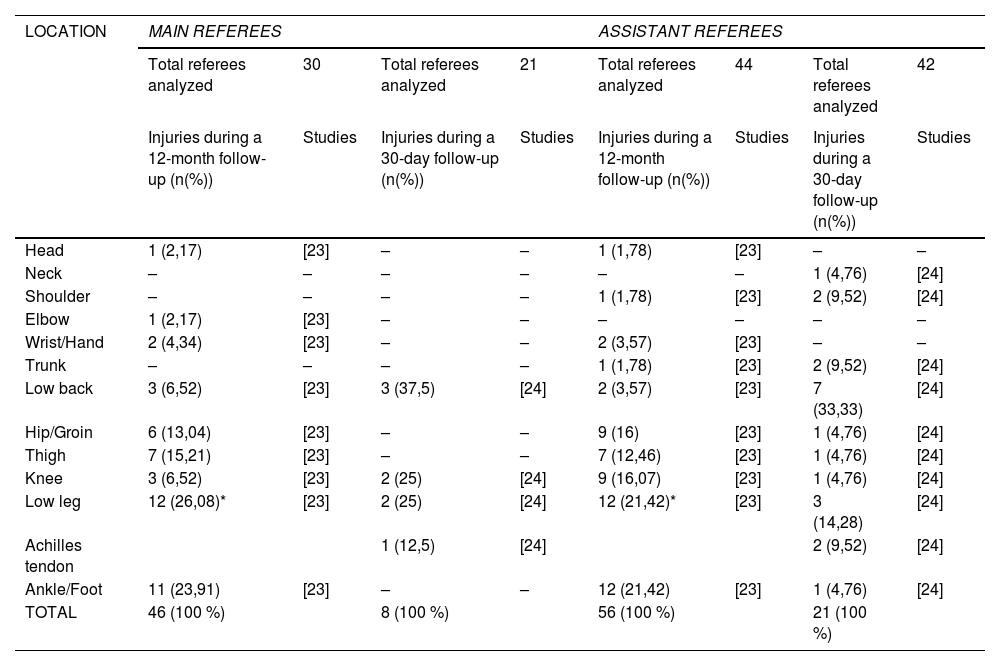
Regarding the incidence of injuries categorized by anatomical location, lower leg and Achilles tendon injuries were together reported as the most incident over a 12-month period for both main and assistant referees. Followed by these, the most frequent injuries were ankle/foot injuries in both types of referees. For a 30-day follow-up period, the most frequent injury was in the lower back for both groups. Table 8 presents the incidence data by anatomical location for both groups of referees.
Incidence of injuries in main referees and assistant referees categorized by different anatomical locations.
Note= *: Lower leg and Achilles tendon injuries were reported together.
Unfortunately, categorization and operationalization of incidence data by diagnosis was not feasible in this context. This limitation arises due to the size of the study population for this category of analysis, which has resulted in all diagnoses receiving an equal incidence percentage.
DiscussionThis study provides the first epidemiological profile of injuries in male soccer referees, using a systematic review methodological design covering a broader population. This approach, previously employed in other populations such as pediatric soccer players11 and ultramarathon and non-ultramarathon runners,28 allows to identify and compare at a global level the most frequent injuries, discriminated by anatomical location or diagnosis.
Differences were observed between main and assistant referees. In particular, injuries to the upper limbs stands out, where the main referees did not report any injury in any follow-up period in terms of prevalence. On the contrary, assistant referees presented shoulder and elbow injuries. In terms of incidence, it was evident that 9.72 % of the total injuries and 1.78 % corresponded to shoulder injuries during a follow-up of 30 days and 12 months. In addition, 3.57 % of the total injuries during a 12-month follow-up period corresponded to hand injuries. A plausible hypothesis is that assistant referees, having to lift and move the flag to signal infractions, are more exposed to repetitive movements of the upper limb with external load, which could trigger shoulder, elbow or wrist injuries. Therefore, the inclusion of specific exercises for the prevention of upper limb injuries in training protocols should be considered, since as far as is known, the only existing protocol to prevent injuries in referees is the FIFA 11+ extension, which does not include specific exercises for this area.29
Also, assistant referees may be more susceptible to knee injuries. Although the percentages were slightly higher in assistants than in main referees, this fact should be taken into account, given that assistant referees rely heavily on their technical skills to move laterally in a safe manner and perform quick changes of direction while following the game. Poor technique in these movements could increase the risk of musculoskeletal injuries,30 such as medial ankle sprains, as well as injuries in the knee ligaments, like the anterior cruciate ligament or the lateral collateral ligament.
It is crucial to pay attention to injuries during the physical tests, as it is observed that the most prevalent injuries for main referees are in the knee, while for assistant referees are in the knee, hip and groin. This could be attributed to the level of demand of the physical tests, particularly the change of direction test for assistant referees, which involves making cuts at high speeds, which could increase the risk of injuries to the adductor musculature and the knee. In addition, although main referees focus more on straight-line speed and cardiovascular endurance, the speed required during these tests may also increase the risk of knee injury due to the impact suffered during running contact.31 Therefore, special attention must be paid to the warm-up program and the initial fitness level to perform the FIFA-regulated tests for the refereeing corps.
Moreover, it is important to recognize the limitations associated with this review. On one hand, it is crucial to mention that, although the inclusion of several studies considerably increases the size of the population, others were excluded during the screening process since they did not report the injuries discriminated between the two types of referees, which could introduce a publication bias by discarding relevant data. However, after attempting to contact the authors, it was not possible to obtain the discrimination by referee type, thus respecting the initial premise that it is not appropriate to mix populations due to differences in physical and psychological requirements during refereeing.
Besides, another important limitation is the lack of specificity in the report of the anatomical location of the injuries in some studies, where general diagnoses such as muscle contractures, tendon injuries or sprains are mentioned, without specifying to which anatomical structure they correspond. This can lead to erroneous conclusions due to the lack of knowledge of the specific diagnosis of each injury. Thus, it is essential that future studies be more specific in reporting the location of the injury associated with the diagnosis. Also, it is important to be aware of recall bias in retrospective studies, especially those that collect data over prolonged periods, which could result in underestimation of injuries.
In summary, the results of this review can serve as a basis for the development of new injury prevention protocols that address all potential injuries presented by both types of referees. Given that the only known program is the FIFA 11+ extension for referees, it is critical to consider referees on a similar plane to players, which urges national decision-makers and international bodies such as FIFA to employ and constantly update policies related to the health of the refereeing corps, thus encouraging research targeting this population. This could not only reduce medical costs, but also promote the vitality of the refereeing corps and ensure a safe working environment.
Finally, it would be interesting in future research to elucidate the differences in the epidemiological profiles of injuries in referees, depending on the soccer league to which they belong or the type of competition in which they referee. Different leagues may adopt game methodologies that involve greater speed. This may require referees to move faster and make decisions in less time. Furthermore, the speed of play may vary according to the level of competition and the league.32 In addition, it would be pertinent to investigate whether refereeing in finals of important competitions requires the same precision and cognitive performance as in regular matches. A higher number of injuries could be anticipated in high-level matches, where championships are disputed, due to the greater cognitive stress to which they are exposed. This aspect is relevant in relation to the ability to perform dual tasks in the context of injury prevention and rehabilitation to avoid second injuries.33
ConclusionThe presence of injuries in the soccer refereeing corps is a reality that deserves meticulous attention. These injuries, diverse in nature and location, can arise at specific times, whether during FIFA-regulated physical performance tests, after refereeing a match or throughout the referee's career. It is critical to understand the variety and severity of these injuries in both main and assistant referees. This differential recognition could be crucial when designing customized injury prevention programs that are tailored to the specific needs of each type of referee. It is therefore imperative to address these concerns with well-defined and tailored prevention strategies, thus ensuring the health and well-being of those who play a fundamental role in the sport of soccer.
None.

