







Complex training (CT) combines resistance and plyometric exercises. It improves athletic performance but also leads to fatigue and muscle damage. Recovery strategies like self-myofascial release (SMF) have gained attention. However, it is still unclear how effective they are when used before and during training.
PurposeThis study looks at the effects of SMF applied before (PMF) and during (DM) CT on recovery. The study used creatine kinase (CK) and Delayed Onset Muscle Soreness (DOMS) as signs of fatigue and muscle damage in football players.
Materials & methodsThe research used a quantitative, experimental design with 36 professional football players aged 20–25. They were randomly divided into three groups: PM (PMF with foam roller + CT), PDM (DM techniques + CT), and a control group (CG) that only did CT. CK and DOMS measured at 0, 24, 48, and 72 h after training. Analysis was done using repeated-measures ANOVA (p < 0.005).
ResultsThe treatment groups (PM, PDM, CG) and the timing of measurements significantly affected CK levels and DOMS. PDM had the lowest CK levels, indicating a significant reduction in muscle damage. This group also reported less soreness compared to the others.
ConclusionUsing SMF before and during exercise effectively lowers CK levels and DOMS, with PDM providing the greatest recovery benefits. These findings suggest that incorporating SMF techniques into training can improve recovery and reduce muscle damage caused by exercise.
Football is one of a sports discipline that require athletes to develop a wide range of physical and neuromuscular attributes and structured movement patterns that support both the explosive nature of the game and its endurance requirements in training and competition.1 It places significant stress on the musculoskeletal system; it requires athletes to perform repeated explosive actions and shift direction rapidly, especially in high-intensity competition. Among the different conditioning strategies, athletes often use complex training (CT), which blends resistance plyometric exercises in a single session, to develop strength, speed, and power.2 This method has been especially suitable for sports like football, where players frequently engage in sudden accelerations, directional changes, and vertical jumps during matches and training sessions. However, while CT supports performance gain, it is also subjects the body to some sort of physiological strain, as the high intensity nature of exercises included in this such as sprinting, jumping, and resistance-based lifting, often induce acute fatigue, elevate muscle damage and soreness after sessions.3 The accumulation of fatigue, inflammation, and muscle microtrauma from CT necessitates effective and timely recovery strategies. Without appropriate recovery, the benefits of such training may be overshadowed by impaired performance, reduced training quality, and heightened injury risk.
Intense CT sessions sometimes leads to Exercise-Induced Muscle Damage (EMID), a condition characterised by microscopic tears in muscles, inflammatory responses, and a cascade of physiological disruptions.4,5 It occurs due to the metabolic and mechanical stress placed on the muscle during exercise, and the accumulation of metabolic by-products due to insufficient oxygen supply during high-intensity exertion, especially during eccentric contractions that overstretch muscles and breakdown muscle proteins and disrupt muscle structure.5,6 These factors compromise muscle integrity and function, causing pain, stiffness, and a reduction in range of motion. One common biochemical marker of muscle damage is creatine kinase (CK), an enzyme that enters the blood stream when the muscle membrane (sarcolemma) breaks down and its levels usually peak 24–96 h post-exercise, depending on exercise intensity and contraction type.7 If not managed properly, this damage can impair subsequent training and elevate injury risk, especially in sports requiring daily or frequent sessions.
To address these challenges, athletes need to depend on variety of recovery strategies such as dynamic warm-ups, post-exercise rest, and cool down routines. Effective warmups, during and post-training rest, and recovery are key for preparing to enhance mobility, reduce stress, and support muscle repair to reduce injuries and boost performance.8,9 Proper activation and cool-down are crucial for preventing muscle damage, minimising fatigue, and enhancing performance.10 One approach in these context that is gaining popularity is Myofascial Release (SMF), which widely used as part of a dynamic warm-up routine to prepare muscles and fascia for the exercise.11 It also alleviate muscle tightness,12 improve flexibility,13 and reduce pain by applying sustained pressure to targeted areas of the body,14 thereby helping the players to perform at their best during training and competition.15 SMF involves using tools like foam rollers, massage balls, and massage guns to apply pressure to the targeted muscles. SMF using foam roller is a widely adopted technique for improving the range of motion,16 reducing muscle soreness,17 perceived pain,18 and risk of injury, fatigue recovery, relaxation, and performance enhancement.19
In high-demand sports like football, rapid repeated actions and explosive movement are common; integrating the SMF can potentially support the performance by eliminating the damage of muscle fibers, delaying neuromuscular fatigue, leading to performance optimisation.20–22 Athletes use SMF intervention during the warm-up routines to prepare muscles for exertion, muscle activation, and injury prevention23,24. Although positive evidences are there like this in the literature, few research highlights that prolonged or excessive SMR (such as 5 min or more) before activity may slightly decrease power output, such as vertical jump performance, which could be detrimental if maximal power is required for the subsequent activity.25,26
While SMF is most commonly used before or after the exercise, a few studies have recently explored the potential of applying it during the exercise session, especially during CT where fatigue accumulates quickly. SMF techniques involve various manipulations like pressure, friction, rubbing, shaking, vibration, and kneading.27 Since ancient times, massage has played a vital role in sports recovery, and is suggested to eliminate the accumulating extracellular fluid from affected muscles by increasing lymph circulation.28 Mechanistically, massage activates signalling pathways that decrease inflammatory mediators such as interleukin-6 and tumor necrosis factor-alpha, while also enhancing mitochondrial biogenesis, which supports muscle repair and adaptation.29,30 It reduces the risk of overtraining injury and helps progression in athletic performance. Massage is also believed to stimulate inflammatory mediators that reduce pain perception and improve movement efficiency. Despite this, limited empirical evidence explores whether SMF during training can attenuate acute muscle damage, as reflected by CK and DOMS levels. This gap suggests the need for a closer scientific examination of intra-session recovery methods that support ongoing performance without interrupting training flow.
Given football’s high physical demands and the dual stress of resistance and polymeric loading in CT, recovery strategies that prevent performance decline and reduce muscle damage markers like CK and DOMS are essential. This study aims to investigate the impact of pre- and during-exercise SMF on CK levels and DOMS in football players undergoing CT, aiming to provide scientific insight into effective recovery protocols. It explores whether inter-set SMF can serve as a valuable tool to modulate fatigue, enhance readiness, and minimise risk of injury during high -intensity training. By addressing this gap, the research seeks to offer practical insights in to optimizing recovery protocols, thereby contributing to better training outcomes and long-term athletic development in football.
Methodology and materialsStudy designThis study employed a randomised, experimental, two-way mixed ANOVA design. A quantitative research design was used to evaluate the effects of pre- and during Myofascial Release (SMF) on recovery after complex training (CT). Participants were randomly assigned to one of three groups, where the Pre-Myofascial (PM) group performed Pre-Myofascial Release (PMF) using Foam Roller (FR) before Complex Training (CT). The Pre-During Myofascial (PDM) group performed Pre-Myofascial Release (PMF) with Foam Rolling (FR) and During-exercise Massage (DM) therapy during CT (inter-set massage) using apothecary and shaking techniques. The Control Group (CG) performed CT without any SMF intervention. Before the intervention began, all participants completed a One-Repetition Maximum (1RM) test on split squats and bench presses to fix the training load. After a general warmup and activation for 10 min, the participants received instructions regarding the 1RM testing protocol. After each successful lift with proper form, the 1RM test involved incremental weight increases (1–10 kg). A failed lift was an incomplete range of motion (ROM) or two consecutive failure attempts. If the participant failed to perform two consecutive tries or they had reached their 1RM, the previous successful lifted weight is considered as 1RM. The participants completed two familiarisation trials before 96 h the intervention began.
ParticipantsThirty-six male football players with at least two years of weight training experience were selected for this study subject characteristics shown in Table 1. The researcher explains the whole details and objectives of the study verbally and in writing, before obtaining the consent. Subjects who had pre-existing injuries and were undergoing rehabilitation were excluded from the experiment. The study received institutional ethical approval from the Pondicherry University health and life science research ethical committee. Participants were randomly assigned to one of three groups (n = 12 each): the Pre-Myofascial (PM) group, which performed Pre-Myofascial Release (PMF) using a Foam Roller (FR) prior to Complex Training (CT); the Pre-During Myofascial (PDM) group, which performed PMF using FR and received During-exercise Massage (DM) therapy during rest intervals of the CT session using apothecary techniques and muscle shaking; and the Control Group (CG), which performed CT without any Self-Myofascial Release (SMF) intervention.
Assessment of creatine kinase (CK)Immediately after the intervention, medical professionals took the blood sample with all the safety requirements. Blood was taken from the antecubital vein to analyse serum Creatine Kinase (CK) following the procedures outlined by prior established researchers.7,31 Blood was collected immediately after the Complex Training (0 h), and subsequently at 24 h, 48 h, and 72 h after the completion of the training.
Assessment of muscle sorenessA Visual Analog Scale (VAS), ranging from 0 to 100, where 0=no soreness, 25=mild, 50= moderate, 75=severe, 100=worst possible soreness. Assessment was conducted at four time points: immediately after Complex Training (0 h), and at 24 h, 48 h, and 72 h post-training. Participants were instructed to refrain from any form of physical exercise and from taking anti-inflammatory medications throughout the data collection period to avoid influencing the results.32–36.
ProcedureSubjects perform 10 min of treadmill or cycle ergometer activity and 15 min of dynamic mobility exercise for the upper and lower body.37 In addition to this general warm-up, participants in the Pre-Myofascial (PM) group and the Pre-During Myofascial (PDM) group performed Self-Myofascial Release (SMF) using Foam Rolling (FR) for 15 min, applying 2 × 15-second bouts per muscle group with adequate rest between sets.38 Foam rolling was directed at primary muscle groups involved in the training exercises, including the quadriceps, hamstrings, glutes, and upper body muscles related to split squats, alternate jump lunges, bench presses, and explosive push-ups.35 After completion of the active warmup, the subject was allowed 5 min of relaxation. All three groups, PM, PDM, and Control Group (CG), performed complex training protocol consisting of: 2 × 6 split squats and 2 × 6 bench presses at 80–85 % of one-repetition maximum (1RM) ,39 followed by 2 × 10 alternate jump lunge, and 2 × 8 explosive push-ups. The PDM group received an additional 10-minute during-exercise massage between the strength and power sets, using apothecary massage and muscle-shaking techniques as part of their During-exercise Massage (DM) protocol.40 Following the training session, Creatine Kinase (CK) and Delayed Onset Muscle Soreness (DOMS) assessments were conducted immediately (0 h), and at 24 h, 48 h, and 72 h post-CT.41 The flow of participant enrolment, group allocation, and intervention sequence is illustrated in Fig. 1.
Statistical analysis
Data normality was assessed using the Kolmogorov-Smirnov test for each dependent variable, Creatine Kinase (CK) and Delayed Onset Muscle Soreness (DOMS), across four time periods (0hr, 24hr, 48hr, and 72hr). A two-way mixed ANOVA was conducted to compare group differences (PM, PDM, and CG), time effects, and the group x time interaction on CK and DOMS levels. Mauchly’s Test of Sphericity was conducted to verify the assumption of sphericity for two-way mixed ANOVA. The test was not violated for the group (p = 0.683), time (p = 0.280), or the group × time interaction (p = 0.116), confirming that uncorrected F-tests could be applied. Bonferroni-adjusted pairwise comparisons were performed for significant F-ratios to identify differences between groups and periods, ensuring statistical robustness. Effect sizes (partial η²) were reported to quantify the magnitude of differences (small = 0.01, medium = 0.06, large ≥ 0.14) .35 All statistical analyses were performed using SPSS (Version 27, IBM Corp., Armonk, NY, USA). Statistical significance was set at p < 0.05, and all values are presented as mean ± standard error (SE) unless otherwise indicated. The DOMS was assessed by VAS, ranging from 0 to 100.34–36
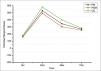
ResultCreatine kinase (CK) responseTable 2 presents the descriptive statistics and comparative outcomes for Creatine Kinase (CK) levels across different time intervals following complex training (CT) across the three groups: Control Group (CG), Pre-Myofascial Release Group (PM), and Pre- and During-Myofascial Release Group (PDM). At 0 h post-CT, the control group (CG) recorded a CK level of 179.83 ± 5.50 U/L, whereas the pre-myofascial release (PM) and pre- and during-myofascial release (PDM) groups showed lower mean scores of 169.75 ± 4.44 U/L and 158.92 ± 4.21 U/L, respectively. At 24 h post-CT, the CG demonstrated a significant increase to 581.00 ± 4.49 U/L, while PM and PDM maintained lower means of 527.67 ± 3.81 U/L and 492.50 ± 4.59 U/L. At 48 h, CK levels decreased to 398.58 ± 5.21 U/L in CG, 345.33 ± 7.06 U/L in PM, and 302.83 ± 5.14 U/L in PDM. By 72 h post-CT, CK levels further declined in all groups: CG to 284.00 ± 3.39 U/L, PM to 269.08 ± 3.44 U/L, and PDM to 254.58 ± 5.16 U/L. These results indicate that both PDM and PM interventions had a greater effect in reducing CK levels compared to the control condition. A significant main effect of PM, PDM, and CG was observed (p < 0.001, partial η² = 0.975), indicating that CK levels varied significantly among groups (PM, PDM, and CG). Similarly, a significant main effect of time (p < 0.001, partial η² = 0.998) confirmed that CK levels changed significantly over time. The group × time interaction was also significant (p = 0.002, partial η² = 0.943), suggesting that group and time influenced CK responses. Mauchly’s test confirmed that the assumption of sphericity was not violated (p > 0.05), allowing for uncorrected F-tests. Bonferroni-adjusted pairwise comparisons demonstrated significant differences across all groups and periods (p < 0.001). Specifically, PM resulted in significantly higher CK levels than PDM (MD = 25.75, p < 0.001), while CG exhibited significantly greater CK levels than PM (MD = 32.90, p < 0.001). CK levels peaked at 24 hours’ post-exercise before declining progressively. The most significant increase occurred between 0 and 24 hr (MD = −364.22, p < 0.001), indicative of an EIMD response. (Fig. 2) display the Creatine Kinase Response Over Time. These findings align with existing literature, which suggests that higher-intensity exercise protocols elicit better CK release, reflecting increased muscle tissue disruption and subsequent recovery demands.
Descriptive Statistics and Analysis of Creatine Kinase (CK) Levels Across Time Points.
Note: PM: Pre-myofascial release group; PDM: Pre-During myofascial release group; CG: Control group.

(Table 3 presents) the descriptive statistics for delayed onset muscle soreness (DOMS) across four time points following complex training (CT) for the pre-myofascial release (PM), pre- and during-myofascial release (PDM), and control group (CG). At 0 h post-CT, the mean DOMS value was 24.38 ± 0.81 for PM, 19.58 ± 0.42 for PDM, and 29.46 ± 0.48 for CG. At 24 h post-CT, the DOMS increased to 43.25 ± 1.96 in PM, 40.50 ± 1.17 in PDM, and 57.17 ± 1.50 in CG. At 48 h post-CT, DOMS values peaked, with PM at 69.00 ± 0.48, PDM at 63.42 ± 0.18, and CG at 73.25 ± 0.29. By 72 h post-CT, DOMS scores declined in all groups: PM to 28.42 ± 0.90, PDM to 26.13 ± 0.36, and CG to 32.75 ± 1.07. These results indicate that both PM and PDM interventions were more effective than no intervention (CG) in reducing DOMS, particularly evident at 24 h, 48 h, and 72 h post-training.
Descriptive statistics of DOMS.
| Period | PM | PDM | CG |
|---|---|---|---|
| 0hr | 24.38 ± 0.81 | 19.58 ± 0.42 | 29.46 ± 0.48 |
| 24hr | 43.25 ± 1.96 | 40.50 ± 1.17 | 57.17 ± 1.50 |
| 48hr | 69.00 ± 0.48 | 63.42 ± 0.18 | 73.25 ± 0.29 |
| 72hr | 28.42 ± 0.90 | 26.13 ± 0.36 | 32.75 ± 1.07 |
Note: PM: Pre-myofascial release group; PDM: Pre-During myofascial release group; CG: Control group.
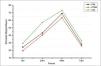
The assessment of DOMS using Visual Analogue Scale (VAS) at four time periods: 0 h,24 h, 48 h, and 72 h post-intervention. At the baseline in 0 h, the PM reported a soreness level of 24.38 ± 0.81 (mild pain); at 24 h, it increased to 43.25 ± 1.96 (mild to moderate); at 48 h, it further increased to 69.00 ± 0.48 (moderate to severe) and at 72 h, soreness decreased to 28.42 ± 0.90 (mild). In comparison, the PDM had a lower baseline in 0 h soreness of 19.58 ± 0.42 (mild pain); this increased to 40.50 ± 1.17 at 24 h (mild to moderate); at 48 h, soreness further increased to 63.42 ± 0.18 (moderate) and the soreness decreased at 72 h to 26.13 ± 0.36 (mild) lowest soreness compare to all groups. In comparison, CG had higher baseline soreness of soreness at 0hr 29.46 ± 0.48 (mild), increased to 57.17 ± 1.50 at 24 h (moderate to severe), reached 73.25 ± 0.29 at 48 h (severe), and then slightly decreased to 32.75 ± 1.07 at 72 h (mild to moderate pain).
A significant main effect of PM, PDM, and CG was observed for DOMS (p < 0.001, partial η² = 0.973), as well as a significant main effect of time (p < 0.001, partial η² = 0.999), suggesting that muscle soreness varied significantly between groups (PM, PDM, and CG) and across time periods. However, the group × time interaction was not statistically significant (p = 0.282, partial η² = 0.621), indicating that while DOMS levels changed over time, the pattern of change was similar across groups. Mauchly’s test confirmed that the assumption of sphericity was not violated (p > 0.05), allowing for uncorrected F-tests. Bonferroni-adjusted pairwise comparisons revealed significant differences across all groups and time periods (p < 0.001). Specifically, CG resulted in significantly greater DOMS levels than PM (MD= 6.90, p < 0.001), while PM elicited significantly higher DOMS compared to PDM (MD = 3.85, p = 0.001). DOMS peaked at 48 hours’ post-exercise before declining, consistent with previous research on EIMD. The most significant increase occurred between 0hr and 48hr (MD = −44.08, p < 0.001), supporting evidence that peak soreness typically manifests between 24–48 h due to inflammatory and repair processes, DOMS response over time is shown in Fig. 3.
DiscussionEffect of SMF on CK
The findings of this study indicate that SMF, when applied before and during the CT, plays a significant role in modulating the CK levels and is a well-established biomarker of muscle damage. Although this result support SMF’s role in aiding physiological recovery, the influence on actual performance or functional capacity should be interpreted cautiously, as no performance-based outcomes were assessed. The result of the study suggests that incorporating SMF as part of the warmup and inter-set recovery strategies positively influences the physiological recovery markers, alleviates muscle fatigue, and may accelerates post-exercise recovery and performance. Pre-exercise myofascial release (PMF) prepares muscle and fascia by enhancing tissue pliability and increasing local blood flow. These benefits reduce passive muscle stiffness and may improve neuromuscular readiness, allowing more efficient movements during high-intensity training. Meanwhile, during-exercise massage (DM) (during the inter-set recovery period) actively promotes the circulation and mechanical dispersion of accumulated metabolic by-products. This mechanism could reduce localised muscle stress and inflammation, thereby limiting muscle fibre damage.
Elevated levels of post-exercise CK reflect muscular micro trauma and increased recovery demand.42 However, the PDM, which received both PMF and DM, exhibited the lowest CK across all the periods, indicating a more favourable muscle recovery trajectory compared to the PM group (PMF only) and especially the CG, which received no SMF intervention. The CK response revealed that levels peaked 24 h post-CT in all groups, a pattern consistent with previous research demonstrating muscle micro trauma following high-intensity resistance and plyometric training.34,43 These findings align with previous studies, which reported that CK levels typically peak at 24 h post-exercise and decrease in 48–72 h, depending on training intensity and recovery strategies.31,44 The control group (CG) exhibited the highest CK concentrations, indicating more significant muscle stress and damage. These outcomes further supports prior evidence that SMF enhances blood circulation, reduces muscle stiffness, and facilitates metabolic waste clearance, thereby mitigating muscle damage.27 Additionally, research on plyometric training-induced muscle damage supports the findings, showing that PM significantly reduces CK levels and improves recovery.7 Notably, the present study highlights that PDM was more effective than PM alone in reducing CK levels, likely due to continues muscle relaxation and reduced tightness during training. These effects may help to minimise fatigue and sustain muscle function during CT. These results support the possibility of SMF during the inter-set by alleviating muscle tightness40,45 and supported by improved blood flow.46
Athletes with greater muscle mass and regular training often exhibit higher baseline CK, when compared to untrained individuals.47 This highlights the need for effective interventions that limits early muscle damage and alleviates the progression of inflammation and tightness during exercise, maintaining muscle tissue in a functional state. Therefore, adopting targeted recovery strategies is essential for maintaining tissue functionality and ensuring optimal performance.20,22 It is important to note, however, the literature represents mixed findings regarding the effectiveness of SMF on CK levels. Some studies have found that SMF (or foam rolling) after high-intensity activity, such as endurance events or explosive sports, accelerates CK reduction and improves muscle recovery compared to passive recovery methods.48 Likewise, other studies have found no significant difference in CK clearance between SMF and passive recovery, particularly when SMF is performed as a single session or in specific populations, such as female soccer players.49 These inconsistent findings may be influenced by factors such as individual variability, SMF duration and timing, targeted muscle groups, or the intensity of prior exercise. Thus, while the present study supports SMF’s role in modulating CK levels, its universal effectiveness remains uncertain and may not apply in all athletic contexts.
Effect of SMF on DOMSThe current study investigated the effect of SMF on DOMS following CT. The finding discovered that the DOMS level peaked 48 h post-exercise, aligning with established timelines for muscle soreness following high-intensity strength training.33,41 The mechanical strain induced by CT, which includes intensive resistance and plyometric exercise, causing substantial stress on the muscle fibers and the musculotendinous junction. This contributes to the increased perception of muscle soreness.7,43
The study found that the group receiving both pre- and during-exercise SMF (PDM) experienced the lowest DOMS level across the post-exercise time points, followed by the PM. At the same time, the control group (CG) reported the highest muscle soreness level throughout the recovery period. These findings suggests that SMF, when used as both a preparatory and intra-set recovery tool hold the potential to alleviate post-exercise soreness. Inter-set SMF plays a critical role in maintaining neuromuscular efficiency, relieves neural tension, relaxes muscles,12,50 and prepares the nervous system for subsequent high-intensity effort.51,52 This effect may also improves training performance and reduces post-workout pain by decreasing muscle stiffness53 and speeding up recovery.45 The findings of this study support previous research suggesting that SMF can be effectively integrated into warm-up and intra-set protocols to minimise CK elevation and DOMS while optimising the activation load and intensity of exercise. However, it is important to note that these findings are based on self-reported soreness and biochemical markers, without any direct assessment of functional recovery or performance outcomes. Thus, any conclusion regarding enhanced muscle function should be approached with caution
Studies states that DOMS is a typical physiological response to high-intensity exercise, characterised by muscle soreness, stiffness, and reduced ROM, typically peaking between 24 and 48 h post-exercise.41 The findings of this study confirm that PDM significantly reduced DOMS levels at all periods, reinforcing the role of SMF in alleviating post-exercise muscle discomfort and promoting faster recovery.27 Evidence suggests that MFR may improve pain, flexibility, and physical function by targeting fascial adhesions, enhancing blood flow, modulating pain pathways, and increasing tissue elasticity.54,55 Some studies report significant reductions in pain and improvements in range of motion and quality of life, particularly in chronic pain conditions like fibromyalgia and low back pain.56,57 Studies also suggests that massage increases muscle temperature, enhances blood circulation, and stimulates lymphatic flow, which reduces inflammation and improves overall muscle function.17,58 In this context compression-based recovery techniques, including massage and compression garments, effectively manage DOMS and perceived fatigue.58 That said, existing literature presents varied outcomes regarding SMF’s effectiveness on DOMS. Some systematic reviews and meta-analyses conducted on non-athletic population highlight that the clinical significance of these effects of SMF can be modest or inconsistent, with some trials showing no greater benefit than control or sham interventions.59–61 These discrepancies may be attributed to variations in study quality, intervention protocols, individual responsiveness, and the specific conditions treated.62 The result of this study supports the findings that PDM is considered an effective strategy for reducing DOMS, followed by PM. At the same time, CG exhibited the highest soreness levels throughout the recovery period.
Limitations & future directionsThe importance of muscle activation in enhancing performance and facilitating quick recovery is evident. While most previous research has looked at using SMF during recovery, few studies have examined its potential benefits when applied before and during training. The findings of this study suggest that this new combined technique can help reduce the increase of CK and DOMS, thus aiding recovery and optimizing performance. This dual timing strategy, which targets both preparatory and intra-exercise recovery phases, may offer a practical advantage in sports that require repeated bursts of intense effort, such as football. As strength and conditioning practices evolve, coaches and athletes need to identify suitable protocols and explore new techniques to improve training results.
The current study has some limitations. The results were mainly based on biochemical (CK) and subjective (DOMS) markers, without functional or performance-based assessments. Therefore, caution is needed when applying the results to all populations and sports. Also, this study did not assess long-term adaptations, differences across muscle groups, or any potential sex-based variations. The sample only included male football players within a narrow age and training range, which limits broader applicability. Factors such as individual training status, tissue density, recovery capacity, and intervention consistency may influence outcomes.
Intercellular enzymes such as CK and inflammatory markers in blood are frequently considered markers of inflammation and skeletal muscle damage, influencing muscle performance recovery17; however these markers alone do not provide a complete picture of functional readiness or athletic capacity. Therefore, future studies should consider integrating performance-based measures such as strength output, movement efficiency, or power metrics, to better evaluate the real-world utility of pre- and during-exercise SMF. Future research can consider of integrating functional performance indicators, such as sprint speed, jump height, or strength output, alongside physiological markers. Investigations should also explore the long-term effects of combined SMF interventions and their relevance across genders, training statuses, and sports disciplines. A clearer understanding of SMF’s time-dependant efficacy, optimal application timing, and its interaction with other recovery startegies could help refine training methodologies, clarify the broader applicability of these techniques, and minimise overtraining risk.
ConclusionThe results provided insightful evidences that the group receiving the PDM intervention consistently had lower levels of CK and DOMS throughout all periods, performing better than both the pre-training group with just the PM and the control group (CG). These findings highlight the value of using SMF as a warm-up technique and a helpful method during training to improve muscle function, speed up recovery, and lessen fatigue. This study also sheds light on the benefits of using SMF during training sessions, a topic that has received less attention in sports science literature. Applying SMF between training sets helps maintain neuromuscular efficiency, reduce muscle stiffness, and keep performance steady during high-intensity training. This suggests that SMF is a versatile and affordable method that can easily fit into regular training routines without interrupting the flow of sessions. Using SMF as a prep and recovery method during training is a promising way to boost athlete performance and reduce exercise-induced muscle damage (EIMD). Coaches, athletes, and sports practitioners should think about including this strategy in their conditioning and recovery programs. Future research should keep examining the physiological mechanisms, long-term changes, and specific applications of intra-session myofascial release techniques across different athletic environments.
Funding statementThis research received no external funding.
Ethical approvalThe study was approved by the Research Ethical Committee of Pondicherry University under approval number HEC/PU/2023/32/03–07–2023.
The authors declare no conflict of interest
Completing this research would have been difficult without the help of many people and organizations, as well as teamwork and encouragement. The research team thanks the football players for their participation, patience, and dedication, which were essential to this study. It also appreciates the coaches and training staff for their help in fitting the research into the athletes' schedules. Additionally, the team is grateful for the guidance and resources provided by the faculty and staff of the Department of Physical Education and Sports at Pondicherry University, which were key in completing this research.

