






The evaluation of muscle oxygen saturation (SmO2) using non-invasive near-infrared spectroscopy (NIRS) technology has been developed in sports performance settings, though few studies have utilized it for injury prevention. This study aimed to assess and correlate bilateral SmO₂ with injury risk during a repeated sprint ability test with change of direction (RSA-COD), using the Cutting Movement Assessment Score (CMAS). Fourteen female futsal players (age 22.5 ± 4.6 years) participated. The RSA-COD consisted of eight 25-meter sprints with COD at 15 m and 3 m, with speed (m·s2) recorded. Additionally, shot accuracy was evaluated using a goal-scoring point system. Knee injury risk was assessed using the CMAS, while NIRS sensors were placed bilaterally on the gastrocnemius muscles of the dominant (DL) and non-dominant (non-DL) legs during the RSA-COD. Bilateral differences were found in SmO₂ data, muscle oxygen extraction (▽%SmO₂), and total hemoglobin (tHb). Additionally, three players (21.4%) showed a high risk of injury, while 10 players (71.4%) had a medium risk at 15 m. At 3 m, three players (21.4%) had a high risk, and six players (42.8%) had a medium risk. The results indicated that ▽%SmO₂ is associated with a higher risk of injury (r= -0.48, p = 0.041) in the CMAS test. Therefore, exploratory study suggests that bilateral differences in SmO2 data may be related to injury risk. Future studies should consider using two NIRS-sensors to detect potential metabolic imbalances between limbs.
Women's futsal is one of the fastest-growing sports worldwide and is regulated by the Fédération Internationale de Football Association (FIFA). In futsal, players are frequently exposed to collisions, impacts, accelerations, rapid decelerations, changes of direction, tackles, and shots.1,2 These actions are inherent to the game, and players must withstand physical demands. This also highlights the need to understand and address the specific injury risks associated with this sport's physical, technical, and tactical demands.3
Knee injuries, specifically rupture of the anterior cruciate ligament (ACL), are common in female futsal players, with a global incidence of 31.9 days of absence per 1000 h of training exposure.4 The ACL injury is considered one of the most debilitating injuries an athlete can experience, potentially affecting their sports career and leading to long-term knee-related issues.5 The higher prevalence of ACL injury in women is attributed to various factors, including anatomical and hormonal differences. These injuries often occur when the knee is near full extension, accompanied by valgus and internal rotation.6 Non-contact ACL injuries increase in the presence of neuromuscular and biomechanical deficits, such as lateral trunk flexion or knee valgus.7,8 These deficits are modifiable through corrective exercise, which has been shown to reduce knee loading and the likelihood of injury.9 In futsal, lateral cutting with a lateral foot plant is a high-intensity movement performed frequently. It is a fundamental movement used to evade opponents, penetrate defensive lines, and gain an advantage on the play field.10
In this context, a qualitative screening tool called the "Cutting Movement Assessment Score (CMAS)" has been designed as a new method that integrates movement biomechanics during cutting maneuvers.11 The CMAS is a qualitative screening tool focused on injury prevention, and compared peak knee abduction moments through three-dimensional (3D) motion analysis, showing a significant correlation (r = 0.796) .12 Although predicting injury risk is controversial and no single screening tool exists, recent years have seen increased attention to movement quality and profiling due to the adaptable nature of movement biomechanics. This contributes to strategies and measurements to improve modifiable injury risk profiles.11 Another key factor to consider in the potential increase of ACL injury risk is the fatigue imposed during a futsal game, which can lead to altered neuromuscular control.4 Peripheral fatigue can affect muscle activation and intramuscular coordination, resulting in poor movement quality during increased loads on the knee joint.13 In turn, these factors can impair the ability to perform movements related to change of direction (COD), especially during successive high-intensity actions,14 for example in repeated sprint ability (RSA) with COD.15
Moreover, muscle oxygen saturation (SmO₂) refers to the balance between oxygen delivery and oxygen consumption within the muscle tissue, providing a real-time indicator of muscular metabolism.16 SmO₂ has been studied to assess performance, but its role in injury prevention and rehabilitation remains little explored. Poor oxygenation may impair performance and elevate injury risk due to insufficient muscle energy.17,18 In this sense, futsal players often exhibit neuromuscular asymmetries related to non-contact injuries.19 Studies emphasize the importance of bilateral SmO₂ assessment, revealing interlimb differences associated with jumping power and neuromuscular deficits.17,20 Furthermore, SmO₂ data can help detect muscle imbalances during exercise.
Currently, for sports scientists, injury risk reduction and performance are key research topics, with an increasing number of technologies and protocols used for athlete screening. Integrating qualitative tools such as the CMAS can help optimize reconditioning processes while strengthening the scientific foundation for injury prevention in women's futsal. However, few physiologists assess asymmetry using SmO2, partly due to gaps in the scientific literature and limited practical application in the field.21 Therefore, conducting research with NIRS sensors could present coaching staff with new methodologies for practical application. The hypothesize is that performance during the RSA-COD test may influence bilateral asymmetries in SmO2 and CMAS in female futsal players. This study aimed to assess and correlate bilateral SmO₂ with injury risk during an RSA-COD, using the CMAS in female futsal players.
Materials and methodsParticipantsFourteen female futsal players (age 22.5 ± 4.6 years, weight 89.8 ± 12.6 kg, height 176.4 ± 7.8 cm, athletic participation 9.1 ± 3.6 years) from the National University (UNA) futsal team competing in first division of Costa Rica (Women’s Premier League) participated in this study. All participants were healthy and met the following inclusion criteria: (1) between 18 and 30 years of age; (2) playing futsal for at least 2 years as a professional player; (3) absence of any lower limb injuries within the last three months; (4) no past severe injury that may affect their lower limbs, and; (5) no use of substances that enhance the acute effect of exercise. All participants signed an informed consent. The tests were performed 48 h after official matches to avoid residual fatigue. This research protocol was approved by the Scientific and Ethical Committee of the University of Extremadura with number of registrations: Number code: 131/2018, and it was in accordance with the principles of the Declaration of Helsinki.
ProcedureA exploratory research study design was methodology used22 . Initially, the coaching staff was contacted, and the players attended a preparatory briefing before the measurements to understand the procedures. Data collection took place during the regular season to make the study as ecologically friendly as possible, and each player completed a familiarization session one week before each test to minimize learning effects. To mitigate the effects of fatigue in the muscle oxygen variables, the assessments were strategically scheduled during the match day +2 or 48-h after matches, allowing for acceptable recovery time. They were conducted consistently on the official futsal sports field, from 6:00 PM to 7:00 PM, one hour before training. Potential confounding factors, such as pre-training intensity, sleep patterns, and nutrition, were monitored, and the same trained evaluators performed all measurements to ensure consistency. Players were instructed to wear appropriate clothing to allow unrestricted freedom of movement. To develop the injury risk profile, each player identified their dominant leg (DL) as their preferred kicking leg and their non-dominant leg (non-DL) as their non-preferred kicking leg. In addition, intra- and inter-observer reliability was assessed to improve the quality of the measurements.
TestingRepeated sprint ability with change of directionAfter a self-directed warm-up, players performed an eight-sprint repeated of 25-meter, composed of different phases: a 15-meter linear sprint that included a 90° COD and a subsequent 3-meter deceleration phase, followed by a 45° COD, concluding with a final straight seven-meter sprint (see Fig. 1). The test ended with a goal shot to assess ball accuracy. Each sprint with COD was alternated between the DL and non-DL, totaling four sprints per side (right and left). Also, after each sprint, a 30-second active recovery period took place, consisting of a light jog back to the starting line (as shown in Fig. 1). Players receive audio cues (i.e., countdown timers) to maintain the prescribed walking speed. Participants assumed a preparatory posture three seconds before each sprint and waited for the starting signal.
 and 3-m (45°) and shot accuracy.")
The selection of 90° and 45° cutting angles was intentional, given that most COD in futsal are typically under 90° (Charron et al., 2020). Furthermore, a study highlighted the increased risk associated with 90° and 45° cutting angles (Dos'Santos, Thomas, and Jones, 2021). To induce significant fatigue through a more abrupt deceleration, the COD was implemented at the 15-meter mark along a straight line (Dos'Santos et al., 2021). A disc cone marker placed at the 15-meter mark was a reference for the final COD point. Participants quickly evaded the marker and accelerated toward the exit gate, i.e. three meters, where they decelerated and COD, followed by a final acceleration over the last seven meters (see Fig. 1). Finally, a futsal ball was placed at the endpoint, and players executed a shot using the same leg with which they completed the movement. Sprint timing was facilitated by a precise timing system using two pairs of single-beam photocells (Cronox, Madrid, Spain) mounted at a height of 0.6 m above ground level. Participants began each sprint from a point 0.5 m behind the first photocell, with their preferred foot positioned forward on a marked line. Players were instructed to complete all sprints as quickly as possible and were given strong verbal encouragement during each sprint.
Cutting movement assessment score (CMAS)The RSA-COD was evaluated using the 9-item CMAS screening tool.12 Four cameras (Sony Corporation, Minato, Japan) were positioned to capture 2D video of lateral motion in both the frontal and sagittal planes. For the CMAS assessment, if athletes showed any deficits on the items, they were assigned a score, with higher scores indicating poorer technique and potentially greater peak knee abduction moments.23 All video footage was analyzed using Kinovea software (version 0.8.15 for Windows, Bordeaux, France), which is free and was used for qualitative screening. The software enabled playback at various speeds and frame-by-frame analysis. Two researchers evaluated and scored each trial of each sprint through video analysis. One researcher has five years of experience in biomechanics for sports sciences. The second researcher dedicated in the CMAS tool assessment for one year and specialized in injury prevention. Raters were allowed to view the videos independently as many times as necessary. Prior to the qualitative assessment, all raters attended a one-hour training session describing how to score cutting tests using the CMAS and how to uniformly establish and agree on “low risk”, “medium risk” and “high risk” with values set in ranges: <3, 4–6 and >7 points respectively. The CMAS was assessed at 4 cutoff points (Right and Left cutting at 15 m and 3 m). Total knee injury risk was evaluated by averaging the CMAS.
Additionally, for this pilot study, intra-rater and inter-rater intraclass correlation coefficients (ICC) were calculated for each CMAS item as well as the overall score. Intra-rater reliability was obtained of Clear PFC braking (k = 0.940), Wide lateral leg plant (k = 0.898), Hip in an initial internally rotated position (k = 0.982), Initial knee ‘valgus’ position (k = 0.901), Inwardly rotated foot position (k = 0.912), Frontal plane trunk position relative to intended direction (k = 0.891), Trunk upright or leaning back throughout contact (k = 0.889), Limited Knee Flexion during final contact (k = 0.935), Excessive Knee ‘valgus’ motion during contact (k = 0.978) and Average (k = 0.924). Likewise, an inter-rater reliability of Clear PFC braking (k = 0.840), Wide lateral leg plant (k = 0.681), Hip in an initial internally rotated position (k = 0.572), Initial knee ‘valgus’ position (k = 0.640), Inwardly rotated foot position (k = 0.721), Frontal plane trunk position relative to intended direction (k = 0.523), Trunk upright or leaning back throughout contact (k = 0.458), Limited Knee Flexion during final contact (k = 0.739), Excessive Knee ‘valgus’ motion during contact (k = 0.698) and Average (k = 0.652).
Ball-Shot accuracyThe ball-shot accuracy was measured using a scoring system where, at the end of the sprint, the player would pick up a futsal ball at the 9-meter mark and dribble it before shooting from outside the 6-meter area. Two cones were placed 1 m from each goal post, creating a 1-meter target area to the goal's left, right, and center (see Fig. 2). Players were instructed that a shot into the side areas would score 2 points, a shot in the center would score 1 point, hitting a cone would earn 0.5 points, and a shot that missed the goal would score no points.

This points system reflects the best shots and ball accuracy24 . Each shot was executed with the leg that COD during the sprint. Finally, it is important to record that shot accuracy was assessed during the recovery time within 30‑sec and the recovery time started after passing through the timing photocells.
Muscle oxygen analysisThe evaluation of local SmO2 was carried out using a NIRS sensor (MOXY, Fortiori Design LLC, Minneapolis, Minnesota, USA) with a sampling frequency of 1 Hz, which is valid for measuring SmO2 (ICC= 0.773–0.992) .16 The NIRS sensor was securely attached to the gastrocnemius muscle (GM) using a black compression sleeve (MojoSport, New Jersey Ave Brooklyn, USA) that fully covered the GM and blocked light, providing an estimated light compression of 15 to 20 mmHg to avoid affecting the SmO2 results.25 The size of the compression sleeve was selected according to the manufacturer's sizing guide. The skinfold thickness at the measurement site was measured using skinfold calipers to ensure it was less than half the distance between the sensor emitter and detector (∼2.5 cm) .26 In all cases, the GM skinfold (8.35 ± 3.4 cm) was less than half the distance between the emitter and detector. All data were obtained in the DL and non-DL.
The guidelines were followed for the data analysis: 1) average values of the SmO2 from the each sprint were used, 2) SmO2 data > 10 % after the last recorded value was excluded, and 3) data showing a 0 % reading were excluded due to apparent signal loss. The data were visible in real-time to the NIRS technology research expert using Bluetooth and were transferred to a Garmin system (Forerunner 735xt, Garmin, Olathe, KS, USA). Each test was analyzed using Excel (Excel 2016, Microsoft Office 365, USA). Likewise, during the RSA-COD, heart rate (HR) was obtained to monitor the exercise intensity of each female player.
Muscle oxygen analysis included the following variables:
- 1.
Raw SmO2 values were obtained for each leg “SmO2_DL and SmO2Non_DL”.
- 2.
Muscle oxygen extraction “▽ %SmO2”27 was determined by the SmO2 decrease in each sprint for both legs.
- 3.
Mean tHb values (g/dL) were recorded during each sprint.
The descriptive data were expressed as means, standard deviations (SD) and Coefficient Variation (CV %). A repeated measures ANOVA test was conducted a post hoc Tukey test was applied to identify changes throughout the RAS-COD. Player code was used as an independent covariate. A paired-samples Student’s t-test was applied to evaluate differences (DL vs. Non-DL) for each sprint, and Cohen’s d was reported as a measure of effect size (ES). In this study, a sensitivity analysis of statistical power was performed, which sets the sample size, the desired power, and the alpha level (α). Assuming a significance level of α = 0.05, it was determined that a sample of 14 participants would provide 80 % power to detect true effect sizes equal to or greater than ES (d) = 0.702. According to power classification guidelines, ES (d)= ≤ 0.464 is “likely miss” (power ≤ 50 %), ES (d) between 0.464 and 0.702 are “good chance of missing” (power = 80 %−95 %), and ES (d)= ≥ 0.930 is “almost surely detect” (power ≥ 95 %).28 This analysis allows to avoid type I errors in the interpretation of the results. Additionally, a multiple regression analysis was performed to identify correlations between RSA-COD performance, injury risk, and SmO2 data, using the DL and non-DL as influencing factors between variables and player code as a covariate. The significance level was set at p < 0.05. All data were analyzed using JAMOVI 2.2 (The Jamovi Project, 2020).
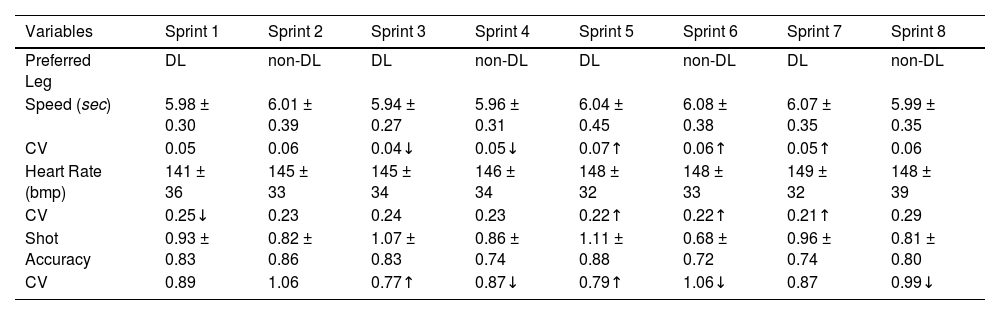
ResultsTable 1 presents the variables description of the speed, HR, and ball accuracy. First, greater speed was showed in sprint-3 compared to sprint-5 (p = <0.001, ES = –0.292, 95 % CI [–0.62 to 0.04]), sprint-6 (p = <0.001, ES = –0.383, 95 % CI [–0.73 to –0.03]), and sprint-7 (p = <0.001, ES = –0.357, 95 % CI [–0.70 to –0.01]). Similarly, greater speed was showed in sprint-4 compared to sprint-5 (p = <0.001, ES = –0.228, 95 % CI [–0.56 to 0.11]), sprint-6 (p = <0.001, ES = –0.320, 95 % CI [–0.66 to 0.02]), and sprint-7 (p = <0.001, ES = –0.294, 95 % CI [–0.62 to 0.04]). For HR, changes were observed starting from sprint-5 (p = <0.001, ES = –0.209, 95 % CI [–0.54 to 0.12]), sprint-6 (p = <0.001, ES = –0.216, 95 % CI [–0.55 to 0.11]), and sprint-7 (p = <0.001, ES = –0.254, 95 % CI [–0.59 to 0.08]) compared to sprint-1.
Description of speed, heart rate and ball accuracy during RSA-COD in female futsal players.
Note. The arrow symbol indicates significant changes (p < 0.05), with the direction of the arrow symbol representing an increase (↑) or decrease (↓) in values. CV = Coefficient of Variation. DL= Dominant Leg, and non-DL= Non-Dominant Leg.
For ball accuracy, more points were achieved in sprint-3 compared to sprint-4 (p = <0.001, ES = 0.368, 95 % CI [0.01, 0.73]), sprint-6 (p = <0.001, ES = 0.598, 95 % CI [0.21 to 0.98]), and sprint-8 (p = <0.001, ES = 0.414, 95 % CI [0.05 to 0.78]). Better scores were also found in sprint-5 compared to sprint-6 (p = <0.001, ES = 0.460, 95 % CI [0.09 to 0.83]). This demonstrated that there are differences between DL (3.96 ± 1.63) vs. non-DL (3.11 ± 1.84), which were not significant (p = 0.060) but showed a moderate trend (ES = 0.632, 95 % CI [0.24 to 1.03]).
Fig. 3 presents the muscle oxygenation data for SmO₂, ▽ %SmO₂, and tHb, comparing the DL and non-DL. Significant bilateral differences in SmO₂ were found in sprint-1 (p = 0.044, ES = 0.657, 95 % CI [0.23 to 1.04]), sprint-2 (p = 0.048, ES = 0.663, 95 % CI [0.24 to 1.05]), sprint-3 (p = 0.045, ES = 0.692, 95 % CI [0.27 to 1.08]), and sprint-4 (p = 0.034, ES = 0.784, 95 % CI [0.36 to 1.18]). SmO₂ differences were observed when comparing sprints 1 to 4 with sprint-6 (p < 0.001, ES = 0.205, 95 % CI [–0.13 to 0.55]), sprint-7 (p < 0.001, ES = 0.146, 95 % CI [–0.18 to 0.48]), and sprint-8 (p < 0.001, ES = 0.176, 95 % CI [–0.15 to 0.51]).

Analysis of bilateral muscle oxygen saturation data during repeated sprint ability with change of direction in female futsal player.
Additionally, lower ▽ %SmO₂, values were consistently observed in the DL compared to the non-DL throughout the RSA, with significant differences in sprint-2 (p = 0.048, ES = 0.701, 95 % CI [0.28 to 1.10]), sprint-4 (p = 0.043, ES = 0.714, 95 % CI [0.29 to 1.12]), and sprint-6 (p = 0.049, ES = 0.699, 95 % CI [0.27 to 1.08]). The higher ▽ %SmO₂ was found in sprint-4 compared to sprint-5 (p < 0.001, ES = 0.220, 95 % CI [–0.12 to 0.56]) and sprint-6 (p < 0.001, ES = 0.215, 95 % CI [–0.13 to 0.55]).
Also, tHb lower values were obtained in sprint-1, sprint-2, sprint-3, and sprint-4 compared to sprint-5 (p < 0.001, ES = –0.200, 95 % CI [–0.54 to 0.14]; p < 0.001, ES = –0.342, 95 % CI [–0.69 to –0.01]; p < 0.001, ES = –0.358, 95 % CI [–0.71 to –0.02]; p < 0.001, ES = –0.318, 95 % CI [–0.66 to 0.02], respectively). The same differences were observed for sprint-1, sprint-2, sprint-3, and sprint-4 when compared to sprint-6 (p < 0.001, ES = –0.248, 95 % CI [–0.60 to 0.10]; p < 0.001, ES = –0.388, 95 % CI [–0.74 to –0.04]; p < 0.001, ES = –0.404, 95 % CI [–0.76 to –0.05]; p < 0.001, ES = –0.318, 95 % CI [–0.66 to 0.02], respectively). Similarly, lower values were found in sprint-1, sprint-2, sprint-3, and sprint-4 when compared to sprint-7 (p < 0.001, ES = –0.407, 95 % CI [–0.77 to –0.05]; p < 0.001, ES = –0.548, 95 % CI [–0.92 to –0.18]; p < 0.001, ES = –0.564, 95 % CI [–0.93 to –0.19]; p < 0.001, ES = –0.478, 95 % CI [–0.84 to –0.12], respectively). Additionally, lower values were observed in sprint-1, sprint-2, sprint-3, and sprint-4 compared to sprint-8 (p < 0.001, ES = –0.508, 95 % CI [–0.88 to –0.14]; p < 0.001, ES = –0.649, 95 % CI [–1.02 to –0.28]; p < 0.001, ES = –0.665, 95 % CI [–1.04 to –0.29]; p < 0.001, ES = –0.579, 95 % CI [–0.94 to –0.21], respectively). These differences were noted on both legs. Finally, there was a significant difference between legs in the first sprint (p = 0.035, ES = 0.772, 95 % CI [0.34 to 1.17]), with tHb being greater in the DL.
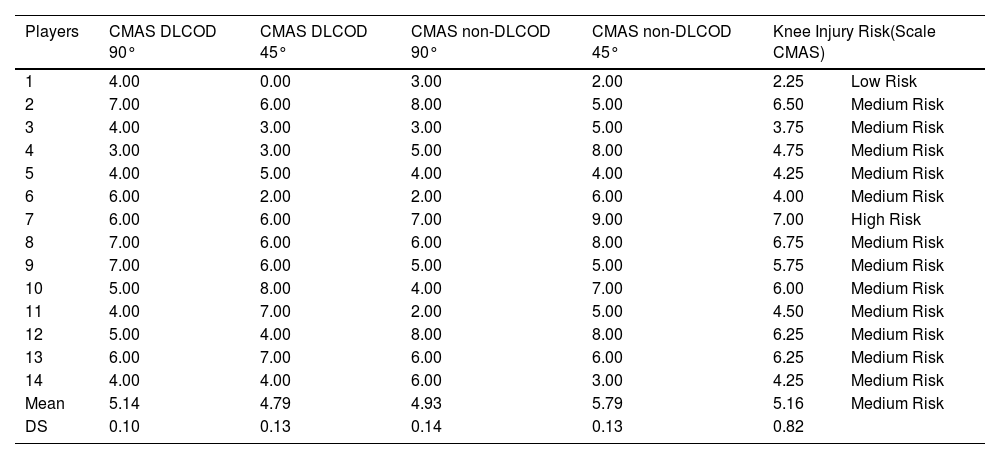
Table 2 shows the knee injury risk obtained from the CMAS during the RSA-COD in female futsal players. A high risk of ACL injury was observed in 3 players (21.4 %) and a medium risk in 10 players (71.4 %) in the COD 90°. Additionally, a high risk of ACL injury was observed in 3 players (21.4 %) and a medium risk in 6 players (42.8 %) in the COD 45°. The high risk of ACL injury in the 3 players in the 15-m was different from that in the 3-m.
Description of knee injury risk through cutting movement assessment during repeated sprint ability in female futsal players.
Note. CMAS= Cutting Movement Assessment Score. CMAS interpretation: low risk= ≤3; medium risk=4 to 6; high risk= ≥ 7 values. COD= Change of direction. DL= Dominant Leg and non-DL= Non-Dominant Leg.
While the non-DL, a high injury risk was observed in 3 players (21.4 %) and a medium risk in 6 players (42.8 %) in the COD 90°. Additionally, a high risk of ACL injury was observed in 5 players (35.7 %) and a medium risk in 7 players (50 %) in the COD 45°.
The total injury risk was lower in the DL (4.96 ± 1.52) compared to the non-DL (5.35 ± 1.70), with a small, non-significant effect (p = 0.181, ES = –0.297, 95 % CI [–0.65 to 0.09]). Similarly, CMAS during the 45° COD was lower in the DL (4.79 ± 2.22) compared to the non-DL (6.10 ± 2.10), with a significant difference (p = 0.043) and a moderate effect (ES = –0.825, 95 % CI [–1.27, to 0.28]). No significant differences were found between legs for the CMAS during the 90° COD.
Fig. 4 shows the correlations obtained from the multiple linear regression analysis. The regression model used ∇ %SmO₂ (dependent variable), ball accuracy, speed time, and CMAS as independent variables (graphs A, B, and C). Speed time was also used as the dependent variable, and CMAS as the independent variable (graph D).

The multiple regression model showed significance and a moderate correlation between variables (r = 0.55, r² = 0.30, p = 0.039, Interceptation β= 46.6, SE=3.77, p = 0.05). In particular, the data show that ∇ %SmO₂ is associated with speed time (β= −15.9 SE= 7.5, p = 0.047; Graph B) and injury risk (β= −6.9, SE= 3.3, p = 0.048; Graph C), which are the significant variables in the model. Ball accuracy does not influence ∇ %SmO₂ for this statistical model (Graph A). Similarly, female players with greater speed had a higher risk of injury (β= 7.4, SE= 0.3 p = 0.003; Graph C).
DiscussionThe main finding of this study shows a bilateral difference in SmO2 data, with non-DL legs obtained greater oxygen extraction during repeated sprints. Furthermore, injury risk and velocity were associated with ∇ %SmO₂. The combined velocity (external load) and muscle oxygen (internal load) data provide information on workload and fatigue tolerance during repeated sprints. Table 1 shows that speed was lower in the sprint-1 and sprint-2 compared to the sprint-3 and sprint-4, but better than in subsequent sprints, where a decrease in speed coincided with the highest HRmax. This can be explained by the fact that once HR stabilization is reached, a reduction in repeated sprint performance begins in female players.29,30 A greater decrease in total time is expected due to repeated COD, since the generation of rapid braking and acceleration forces imposes a greater muscular demand than continuous linear running.31 Therefore, the mechanisms of COD may increase fatigue susceptibility, making it ideal for observing values of repeated sprint decrement.31
In this sense, the gradual decrease in performance during the repeated sprints may have adversely affected kicking accuracy at goal (see Table 1), particularly impacting the non-DL. This decline in accuracy is probable due to the central nervous system's increased difficulty in maintaining intramuscular control and efficiently coordinating movements.32 Adequate acceleration and deceleration of the proximal-distal joint chain are vital for both rapid and accurate ball kicking.32 However, utilizing the non-DL frequently results in movement sequencing errors among player football.33 This accuracy decrease may be related to physiological changes in muscle oxygenation (Fig. 3), as differences were observed between the initial and final sprints, particularly from sprint-4 onward, where a trend of decreasing SmO2 and increasing tHb emerged. This pattern aligns with previous research suggesting that accumulated fatigue during RSA affects the predominance of the energy system.30,34 A decrease in intramuscular partial oxygen pressure (iPO2) leads to immediate desaturation in the first sprints, increasing reliance on the phosphocreatine (PCr) and glycolytic systems before oxidative phosphorylation becomes dominant, triggering an increase in blood flow due to the hyperemic response. This process plays a key role in removing and buffering H+ ions and replenishing intramuscular PCr; however, the accumulation of inorganic phosphate (Pi) during high-intensity sprints results in reduced muscle oxygen utilization.34,35 Notably, a ∇ %SmO2 pattern of a greater increase, suggesting enhanced blood flow and oxygen transport.27,36 This physiological adaptation may contribute to the observed differences in kicking accuracy between the DL and non-DL.
The CMAS (Table 2), most players exhibit a moderate injury risk in the total score, with only one classified as high risk and another as low risk, showing variations in COD 90° and COD 45°. The overall injury risk is lower in the DL (CMAS = 4.79) compared to the non-DL (CMAS = 6.10) at COD 45° but not at COD 90°, which aligns with previous studies indicating that during a 15-m sprint with COD 90°, players have more time to decelerate and adjust their posture, allowing better technical adaptations.37 Conversely, in shorter distances (3 m) with sharper angles (45° to 135°), COD is more abrupt, offering less time for deceleration and body reorientation,38 making motor control key for maintaining stability. Performing COD on the DL may facilitate faster adjustments due to greater motor control, improving the ability to generate and absorb forces efficiently.39 Dominance-related differences, principally in the transverse plane at the knee joint, suggest that the dominant limb exhibits superior force absorption and propulsion during cutting tasks.39,40 In explosive movements, shorter deceleration distances may require a lower center of mass (COM), increased hip flexion, smaller knee angles, and larger internal foot angles, optimizing braking efficiency,11,41 while posteriorly directed braking forces help reduce impulse and enable more effective deceleration for faster cutting.41 Given the repeated sprints and continuous decelerations, fatigue in antagonist muscle groups, in the hamstrings, could impair sensory and proprioceptive function, increasing muscle imbalance and knee injury risk,42,43 possibly contributing to lower CMAS scores and reduced goal-scoring accuracy.44 Additionally, a player’s deceleration technique directly influences the subsequent directed impulse in COD, with the "by-pass" maneuver several short steps used to maintain running speed while widening the COD angle, commonly observed at sharper angles, specifically 45° and 135°38, further highlighting the biomechanical and neuromuscular demands placed on players during rapid directional changes.
Fig. 2 shows that ∇ %SmO₂ was associated with injury risk, as referred to as "CMAS". Therefore, the use of a NIRS sensor could be a strategy to monitor metabolic changes in the female players, in addition to providing information on muscular imbalances in team sports17. The sprint time was related to a lower ∇ %SmO₂, which impairs sprinting ability27,34. Moreover, a recent study reported that angular velocity (s/°) and the impact knee force during high-intensity running were associated with an abrupt decrease in SmO₂,45 supporting the idea that the higher ∇ %SmO₂ observed during RSA-COD may be explained by transient blood flow restriction resulting from high eccentric braking forces and increased muscle oxygen demand during rapid re-acceleration. These findings highlight a close relationship between high running velocity and interlimb muscle oxygen imbalances. Furthermore, as a metabolic variable, SmO2 and ∇ %SmO₂ does not appear to be directly related to ball accuracy in passing and shooting. Although this remains speculative given the nature of the present study, it is noteworthy that this is the first attempt to correlate these variables to explore the potential interaction among repeated-sprints fatigue, ball technique with muscle oxygenation.
LimitationsThis exploratory study analyzed the possible interaction of muscle oxygenation with injury risk during repeated sprint ability with COD performance and ball accuracy in female futsal players. However, the study’s limitations provide insight for improving future research designs. First, more rigorous injury risk control, including inertial sensor and EMG data, could better identify neuromuscular activation levels during repeated sprints. Additionally, pre-test assessments to determine muscle fatigue levels, such as tensiomyography, would be beneficial. The use of data solely from the gastrocnemius muscles, excluding the quadriceps and hamstrings, may limit the physiological understanding of changes in blood flow and oxygen levels. Currently, however, no NIRS sensors allow simultaneous multi-muscle monitoring. Furthermore, reliability and validity studies are needed to assess the use of NIRS in identifying muscle fatigue during sports actions, as NIRS has potential in these investigations.
The COD protocol should be more rigorous, and athletes may need better feedback to perform the turning maneuver effectively. While a 45° turn may lead to 135° turning actions, potentially more effective for avoiding immediate opponent pressure in the sharper 135° turn creates faster separation and drastically changes direction, making it harder for the defender to react. This could explain the difference between CMAS at 45° and 90° Indeed, a previous study showed that the larger the angle, the greater the need to reduce body momentum and apply lateral forces to turn.46
This study concludes that there are interlimb differences in muscle oxygenation, revealing that the non-DL leg exhibited greater ∇ %SmO₂ during repeated sprints and a higher CMAS score in female futsal players. Although the CMAS tool is qualitative, it could be associated with a higher risk of knee injuries. Furthermore, two NIRS sensors are suggested to identify metabolic imbalances between the legs. Finally, encourages sports scientists to expand the methodology, applying these tests to futsal players or adapting them to other team sports.
Funding detailsThis research is funded by postdoc- toral researchers under the Ministerio de Ciencia, Innovación y Uni- versidades del Gobierno Español, supported by the Margarita Salas Program (MS-25).
Data availability statementThe data that support the findings of this study are available upon request from the corresponding author.
Authors contributionsAll authors collaborated in the initial discussions of the topic and drafting the preliminary structure of the manuscript. AAVB was responsible for the initial drafting of the article, which was reviewed and edited by all authors. All authors were involved in the conception, design, and writing. All authors read and reviewed the manuscript critically for important intellectual content and approved the current version of the manuscript.
None of the authors has a conflict of interest to declare.
None to disclose.

