



The ACL injury is considered one of the most serious injuries and usually occurs in actions that include movements with changes of direction, jump and landing. It is a common injury between the young active population and the risk in women of suffering from non-contact injury is superior to that of men. Athletes who suffer from non-contact injuries of the ACL usually have common biomechanical profiles, with landings with large values in ground reaction force (GRF) and therefore, low cushioning on landing.
ObjectiveTo determine possible correlations between GRF and muscular activation at lading after a jump.
Material and methodsThe type of study carried out is an observational study in which, using surface electromyography (EMG), a force platform and an electrogoniometer, the aim is to assess muscle activation and its relationship with GRF (specifically the vertical component Fz).
ResultsCorrelations have been observed between the reaction force of the soil (Fz) in the moments where the reaction force of the soil is greater and the instant where the knee reaches maximum flexion after landing, with the activation of certain muscle groups and differences depending on the gender of the subject.
DiscussionThe neuromuscular recruitment strategies in the phases of maximum GRF load and knee flexion are different depending on the sex of the individual, so it should be considered when scheduling prevention and recovery work.
ConclusionThe evaluation of GRF and muscle activation patterns, allows to assess the dynamics of landing after a jump and to be able to detect different patterns according to sex, with the consequent importance that it can have in the injury mechanism.
Knee injuries and specifically ACL injuries are prevalent in a wide variety of activities (competitive or not) and especially in those that include acceleration-deceleration movements, changes of direction, jump and landing. They are common among young active population1 and the risk in women of suffering the non-contact injury is higher than that in men,2–10 twice,1 five times11,12 and up to six or seven times more13,14 or greater. Athletes who suffer from non-contact injury of the ACL, usually have common biomechanical profiles, with landings with large values in GRF and therefore, little cushioning at landing.15,16
In the field of sports, ACL injury is one of the most common and most serious knee injuries, along with meniscal injury.17–22 Although the actual incidence of ACL injuries is not fully known, it can be estimated through ACL reconstructions that are performed a year before an injury, these are placed on a fork between 200,000 and 350,000 a year in the USA alone23–29 and in 38 out of every 100,000 inhabitants in Denmark,30 one third affecting women.28
The ACL injury is multifactorial (neuromuscular, biomechanical, anatomical, genetic, hormonal, etc.). Although it has been studied, little is known about why the structural weakness of the ligament. The importance of this aspect is that the external forces acting on the tissues also depend on the intrinsic properties of each. And the hormonal aspect can modify these structural properties making it vulnerable to external loads. Therefore, risk factors may also differ depending on gender.31
In the analysis of a jump, the landing phase is of vital importance and a clear example of them is that 31% of the injuries occur on the landing after a jump,32,33 so it is a moment of activity that deserves to be thoroughly studied.
Descriptive studies of non-contact ACL injury indicate that the injury occurs shortly after initial landing contact or after deceleration, with minimal or no contact in 70% of cases.32,34,35
In a normal landing pattern, the muscles contract to absorb the forces of GRF (ground reaction forces) but there may be an abnormal absorption of GRF32,36 and an example of this is that the ischiocrural muscle activity during landing it can vary between 20% and 60% of the value of the maximum voluntary contraction.37
During landing, hip, knee and ankle actions help absorbing reaction forces from the ground. When these segments are not effective in the synergistic work of absorbing GRF, the leg acts as a column of two segments, which sometimes makes it unable to absorb the force of GRF.38 In this same landing activity after a jump, the traction and torsion forces are increased in the ACL with the increase of the ground reaction forces (GRF) and the decrease of the hip angles38,39 and one more straight position, it is associated with an increase in GRF.38,40,41 A landing with a more flexed trunk and an increase in hip and knee flexion can reduce GRF.38,40,42
In relation to muscle strength, a reduction, as well as a reduction in muscle preactivity prior to contact with the ground during sports activities, are factors related with an increased risk of ACL injury in female athletes. Maximum voluntary strength and pre-activation do not have a direct relationship and therefore a person with little muscle strength does not necessarily have to have a bad pre-activation. In order for this pre-activation to be effective, these muscles have to co-activate quickly and adequately since the latency of the feedback sensor reflex is greater than 75–100ms.43–45
Pre-activation is considered important because the ACL lesion occurs 40ms after contact of the foot with the ground at reception after a jump (the GRF peak occurs 40ms after contact with the ground)45–51 being the axial compression force of the knee during landing, 6 times the body weight52,53 and the reason for this may be that a power imbalance between external forces and muscle contractions may partly explain why the injuries of ACL does not usually occur in the window of less than 40ms. Since the foot contacts the ground.43,51,56 Some authors extend this period of time, indicating the range between 30ms and 100ms of the initial contact of the foot on the ground.28,46,51,52
The posterior kinetic chain muscles are especially important: gluteus maximus and medius, hamstrings, and grastrocnemius and soleus. The muscles of the posterior chain must be recruited correctly in order to absorb the GRF; otherwise it will be the ligaments and the joint who should do it. The gluteus maximus, the second strongest muscle in the human body, is the only tri-axial plane controller of the femoral position. When an athlete primarily contracts his quadriceps and reduces the contraction of the gluteus and hamstrings, the result is the collapse of the knee in valgus. And this can be problematic because this allows the GRF to act in a valgus position54 and epidemiological studies indicate that a large knee abduction moment, large knee abduction angles, and the GRF are important predictors of ACL injury risk with 78% sensitivity and 73% specificity.52,55
Neuromechanically, reflex learning regulates joint stiffness and it has been suggested that these mechanisms are centrally pre-programmed (CNS)56–59 and it is not clear whether these pre-programmed activation patterns can be voluntarily changed. Voluntary changes at this level are difficult to achieve.56,60 However, on the external or internal focus of attention, changes in the landing mechanisms have been proven, suggesting that a conscious adaptation of control of pre-programmed landing patterns could be possible.56,60,61 From the neuromechanical point of view, joint stabilization is achieved during voluntary movements with compensatory and anticipatory adjustments to minimize unpredictable and predictable disturbances.61–64 For this reason, we can observe abnormal responses to predictable and unpredictable disturbances in ACL patients, years after the injury; This could mean functional instability during activities of daily living61,65–67 and therefore, an increased risk of re-injury.61,68
For this reason, it is considered important to evaluate the relationship between GRF and the activation of different muscle groups during landing after a jump and see if sex can be a variable that influences these activation patterns. This information can be useful for the evaluation of risk factors, as well as for the programming of activities with preventive purposes in specific populations.
Material and methodsMaterial- -
Biopac model MPC 150 was used to capture the biomedical signals.
- -
For the recording of the electromyographic activity, 4 EMG2-R wireless modules from Biopac were used to collect the signal from the Bionomadix BN-TX model Biopac transmission modules
- -
The RX130B electrogoniometer from Biopac was used to record the goniometry
- -
For the registration of the reaction force of the soil, the piezoelectric platform of forces AMTI brand, USA model SGA6-4 was used
- -
The surface electrodes used were bipolar (Ag/Ag Cl Blue Sensor N-00-S Medicotest)
- -
Abrasive gel, conductive gel. alcohol and cotton were used to prepare the skin
- -
Hypoallergenic adhesive (Hypafix 10cm×10m) was used for electrogoniometer fixation
- -
The validity and reliability of the instruments used is assumed and proven by the manufacturer and his technical department. On the other hand, these instruments have been used in different studies to obtain the results required.70–74
The type of study carried out is an observational study in which, using surface electromyography (EMG), a force platform and an electrogoniometer, the aim is to assess muscle activation and its relationship with GRF (specifically the vertical component Fz), having as main objective to analyze the correlation of activation of the different muscles and the ground reaction force (GRF) detected.
The subjects who have participated in the study are healthy subjects, both sexes, aged between 18 and 30 years and without any pathology or disease that can influence on the balance. Subjects that report an ACL lesion have also been ruled out.
They have also been excluded from the study all those subjects who report having some type of injury or sequel that does not allow them to perform a jump normally or that the jump may be contraindicated with their injury or pathology. Therefore, the study included 74 subjects of which 35 (47.3%) were women and 39 (52.7%) men, with a median age of 23.1 years, a median height of 1.73m and a median weight of 69.37kg (see descriptive data of the study population in Table 1).
Selection criteriaThe inclusion criteria for incorporating subjects into the study were an age between 18 and 30 years old, both genders, being healthy and the acceptation in participating in the study by signing the informed consent. The exclusion criteria were being pregnant, having any pathology or disease that can influence on balance, previous or current ACL injury, having some type of injury or sequel that does not allow them to perform a normal jump or any contraindication of jumping.
Ethical considerationsThe approval for the completion of this study was requested from the Ethics and Research Commission of the Blanquerna School of Psychology, Education and Sports Sciences of the Ramon Llull University. The favorable resolution was obtained on January 17, 2018.
To the subjects, once their participation was accepted and the informed consent signed, a small file was opened in which the personal data were recorded, as well as relevant data for the study (history and clinical history). Once these data were collected, the skin was prepared where the EMG electrodes were to be placed (cleaning and shaving if necessary). The electrodes were as described by Cram and Casman69 in the following muscle groups: quadriceps (vastus medialis and vastus lateralis); hamstrings (semimembranous/semitendinosus and biceps femoris); tibialis anterior; gastrocnemious; gluteus maximus; gluteus medius.
Likewise, the electronic goniometer was placed on the dominant limb, following the alignment of the limb and adhering it to the skin by a hypo-allergenic adhesive plaster. Once the electrodes and electro goniometer were placed, a check was made to ensure that the receivers emitted information and from that moment a new calibration of the electro goniometer was performed, in supine position and sitting; also, the goniometer was calibrated prior to use. Once the initial checks had been made, the baseline data (supine and standing) and maximum contraction values of the groups involved were acquired. The acquisition of the maximum contraction values was made and the subjects were placed on the force platform and their static position was assessed in the 3 axes.
For the election of the dominant side, subjects were asked to kick a ball as they normally would do (they were not given more information) and introduce it between two cones separated from each other by 1.5m and located 4m. The leg chosen for the kick would be considered dominant.
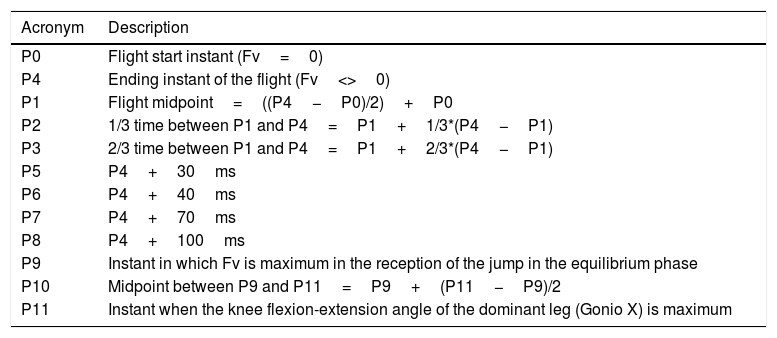
Once this data was collected, we start with the jumps. For this, the subjects were asked to climb on a 45cm high stool and located 35cm away from the edge of the platform. From this initial position and following the indications of the research team, the subjects were asked to jump with both legs on the platform and as soon as they touched the platform, make a vertical jump (the largest possible that would allow them to stabilize later) and land on his dominant leg and stabilize the position, keeping it until they were told it was necessary (see Fig. 1 and Table 2).

Description of the moments of the jump and landing.
| Acronym | Description |
|---|---|
| P0 | Flight start instant (Fv=0) |
| P4 | Ending instant of the flight (Fv<>0) |
| P1 | Flight midpoint=((P4−P0)/2)+P0 |
| P2 | 1/3 time between P1 and P4=P1+1/3*(P4−P1) |
| P3 | 2/3 time between P1 and P4=P1+2/3*(P4−P1) |
| P5 | P4+30ms |
| P6 | P4+40ms |
| P7 | P4+70ms |
| P8 | P4+100ms |
| P9 | Instant in which Fv is maximum in the reception of the jump in the equilibrium phase |
| P10 | Midpoint between P9 and P11=P9+(P11−P9)/2 |
| P11 | Instant when the knee flexion-extension angle of the dominant leg (Gonio X) is maximum |
For this, the necessary number of jumps were made until 3 good jumps could be obtained. They were considered good, all those that the subjects were able to stabilize, landed inside the platform and were unipodal.
Statistical analysisA descriptive analysis was carried out for all the variables collected in the DCN (data collection notebook). Prior to the analysis, the Shapiro Wilks and Kolmogorov–Smirnov tests were performed together with the QQplot graphs to determine the normality of the variables studied. For the majority of the data, clear violations of the normality in the distribution of the data were observed, so it was decided to work according to a non-normal distribution. To study the relationship between variables, the non-parametric linear correlation between variables was used using the Spearman correlation coefficient statistic. The analyzes were performed based on the available dates, without using absent value substitution techniques, and describing the number of missing data for each analysis. In all statistical tests performed a significance level of 5% was used (P value=0.05). All analyzes were carried out with the SPSS v.25 program.
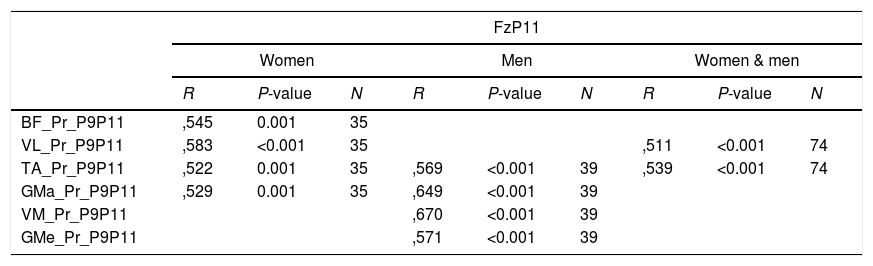
ResultsOnce the results obtained have been analyzed, significant differences have been observed in P9–P11 interval. The P-value, it always been <0.001. As can be seen in Table 3, at instant P11, there is a strong correlation (R) between the reaction force of the soil (Fz) with average activation between instants P9–11 of the vastus lateralis (R=0.511) and tibialis anterior (r=0.539) muscles. In the case of women, at instant P11, there is a strong correlation (R) between the reaction force of the soil (Fz) with average activation between instants P9–11 of the biceps femoris (R=0.545), vastus lateralis (R=0.583), tibialis anterior (R=0.522) and gluteus maximus (R=0.529). On the other hand, in relation to the ground reaction force at instant P11, there is a strong correlation (R) with the activation averages of the vastus medialis (R=0.670), tibialis anterior (R=0.569), gluteus maximus (R=0.649) and gluteus medius (R=0.571) muscles.
Correlation between Fz and muscle activation in the P9P11 interval.
| FzP11 | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Women | Men | Women & men | |||||||
| R | P-value | N | R | P-value | N | R | P-value | N | |
| BF_Pr_P9P11 | ,545 | 0.001 | 35 | ||||||
| VL_Pr_P9P11 | ,583 | <0.001 | 35 | ,511 | <0.001 | 74 | |||
| TA_Pr_P9P11 | ,522 | 0.001 | 35 | ,569 | <0.001 | 39 | ,539 | <0.001 | 74 |
| GMa_Pr_P9P11 | ,529 | 0.001 | 35 | ,649 | <0.001 | 39 | |||
| VM_Pr_P9P11 | ,670 | <0.001 | 39 | ||||||
| GMe_Pr_P9P11 | ,571 | <0.001 | 39 | ||||||
Acronyms and abbreviations:
BF: electromyographic value of the biceps femoris.
Fz: vertical component of the ground reaction force.
GMa: electromyographic value of the gluteus maximus.
GMe: electromyographic value of the gluteus medium.
P9–P11: interval between P9 and P11.
R: correlation coefficient.
TA: electromyographic value of the tibialis anterior.
VL: electromyographic value of the vastus lateralis.
VM: electromyographic value of the vastus medialis.
In the rest of the moments or intervals of the jump and landing, no significant differences were found.
DiscussionThe muscular activity and the correlation in the activation of the different muscles, is an aspect that has been commented by many authors since it is considered important for the prevention of ACL injuries. These muscle correlations tell us about the ability to “work together” and to achieve a good body stabilization after an activity like as in this case, the landing after a jump and to counteract the ground reaction forces (GRF) and thus avoid or decrease a potential risk of injury. There are different authors who point out that there are biomechanical profiles that relate high GRF values with little damping and therefore with a higher risk of injury.
In this sense, the results obtained show that, during the entire jump and landing phase, there are have only found significant differences in the period P9–P11 being P9 the point where the reaction force of the ground is greater and P11 the moment where the knee reaches the maximum flexion after landing. The fact that the differences have occurred in those instants and intervals, supports the idea that, beyond the instants in which the different authors point out that in which the injury normally occurs (interval between P6 and P8), the neuromuscular activity and co-contractions continue to stabilize the joint and allow the individual to continue with the activity or the consequent movements that will occur.69–77 The significance of the practical application of the results is that these results will allow to evaluate in more detail these phases of the landing and give more importance to the late stabilization phase after a jump, giving value to this final phase of stabilization, which even if it is not the phase in which the injury usually occurs, it is necessary to chain activities that occur in sports practice; normally the activities are continued activities, not isolated actions. And so, it is important a good stabilization after each action and that will allow to continue with the activity without injury. And this phase of the landing will be important to consider when planning prevention work as well as when the patient is being rehabilitated.
Regarding with this, it can be noted that there is a high correlation of the activation of certain muscle groups with the GRF in P11; in the case of women, there is a strong correlation with that point with the activity of the biceps femoris, vastus lateralis, tibialis anterior and gluteus maximus muscles at that point P11, while in the case of men, the muscles are vastus lateralis, tibialis anterior and gluteus medius. The muscles of the posterior chain have been previously indicated as essential for the stabilization and absorption of GRF.54 And of course, the co-contraction with the muscles of the anterior chain is necessary for the joint stabilization. On the other hand, also shows the differences that previously have been mentioned in results, in which it is been highlighted the greater activation by women in the gluteus maximus, and the gluteus medius being more active in men. This also agrees with what other authors have indicated; that the mechanisms and reasons for injury may be different depending on sex.31 This will be important to consider when planning the training and prevention exercises, because this could help to reduce the incidence of injuries.
These results lead to conclude that, as other authors point out, depending on sex, there are different neuromuscular mechanisms to face an action such as landing after a jump and this justifies the importance of knowing what are the patterns of activation to prevent an important injury as the ACL injury is but not only in the moment where the injury occurs. It is also important to point out the different use that the subjects do of the gluteus maximus and gluteus medius (two very important muscles for their stabilizing and locomotion capacity), depending on the sex, in this late stage of stabilization.
As a possible methodological limitation of the study, it should be noted that the possible muscular or psychological fatigue that the subject presented by activities done in the previous days, was not considered.
Therefore, for future studies, the fatigue will be considered, because it is believed that it can play an important role in neuromuscular patterns. And of course, it is considered important to study and analyze in more detail the differences in neuromuscular pattern that may occur due to sex.
In conclusion, the evaluation of GRF and muscle activation patterns, allows to assess the dynamics of landing after a jump and to be able to detect different patterns according to sex, with the consequent importance that it can have in the injury mechanism.
Conflict of interestThe authors declare that they don’t have any conflict of interest.

