





Muscular hernias in the lower limb are a rare entity that have seldom been described in the literature, from 1929 about 200 cases of muscle hernias have been described.
CaseHere, we present a case of tibialis anterior muscle hernia and discuss the aetiology behind the same. Furthermore, we attempt to amalgamate existing knowledge to provide some guidance for investigation and management of this important diagnostic consideration.
ConclusionLower limb hernias are rare but should be considered as a differential for unidentified lower limb swellings. There is no clear consensus in literature about treatment, so every case must be individualized.
Las hernias musculares son raras, donde se evidencian con más frecuencia son en las extremidades inferiores siendo el tibial anterior el músculo más afectado. En este artículo describimos un caso de hernia muscular de tibial anterior y su evolución clinica, además de revisión de la literatura actual sobre el tema.
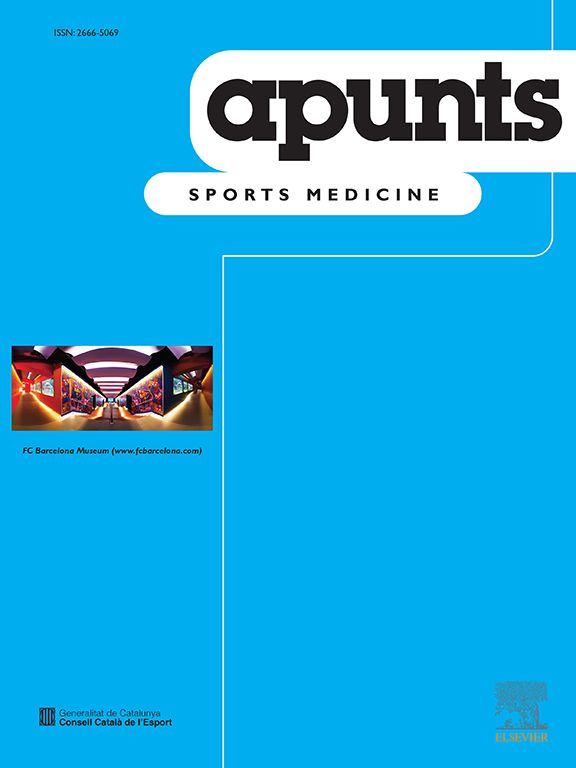
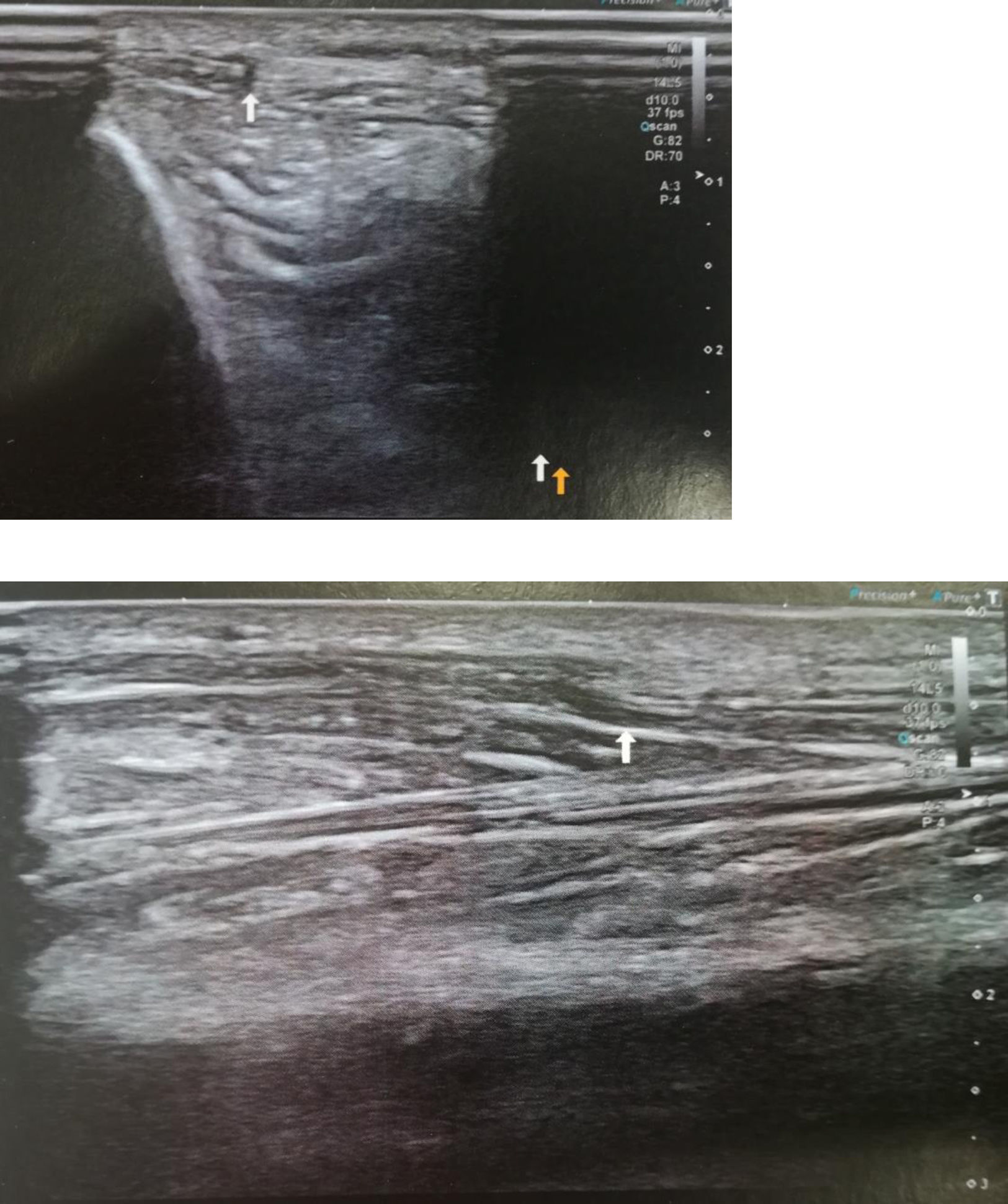
Material y métodosPaciente de 34 años, albañil, que en contexto de accidente laboral (caida de 2 metros) presenta contusión en cara lateral de pierna derecha con diagnóstico de fractura de 1/3 medio de perone de pierna derecha, Paciente presenta buen curso clinico con consolidación completa de la fractura a los 3 meses de evolución, pero persistiendo dolor y aumento de volumen en cara anterior de la pierna. Se solicita resonancia magnética de pierna que es informada como normal. A la exploración en reposo nada a destacar, en bipedestación (Fig. 1) se observa masa palpable de 2 cm aprox en cara anteromedial de 1/3 medio de tibia de pierna derecha, que se reduce al pasar a decúbito supino. Se realiza ecografia dinámica con paciente en bipedestación y forzando dorsiflexión del pie, confirmándose hernia de músculo tibial anterior con disrupción parcia de su fascia, hernia de 11,7 mm de tamaño con 3 cm de extensión (Fig 2). Se realiza tratamiento conservador mediante tratamiento rehabilitador antiinflamatorio (magnetoterapia) + vendajes compresivos locales.
ResultadosPaciente presenta buena evolución clinica presentando a los 4 meses de iniciado el tratamiento disminución de dolor y refiriendo ausencia de hernia, que se confirma a la exploración clinica. Paciente retorna a su actividad laboral sin incidencias.
Comentarios y conclusionesLas hernias musculares son raras, su localización mas habitual es en extremidades inferiores. Son un diagnóstico de exclusión, que muchas veces pasa desapercibido (1) y pueden ser causa de dolor y aumento de volumen crónico unilateral en extremidad inferior.
Muscle hernias of the extremities are most commonly seen in the leg and affect mostly the tibialis anterior muscle. They occur as a result of a defect in the fascial sheath of the muscle secondary to trauma or due to constitutional causes. Most of symptomatic patients usually present with chronic leg pain and occasionally with soft tissue swelling. The diagnosis is challenging as the swelling disappears at rest and reappears during muscle straining. This finding suggests the diagnosis of this entity. Imaging, especially dynamic ultrasonography, plays the most important role in making the diagnosis.
Statement of informed consentThe patient was informed and agreed that data concerning the case would be submitted for publication.
Case report34-Year-old patient, bricklayer, who in the context of an accident at work (2-m fall) presented with a contusion on the lateral aspect of the right leg with a diagnosis of fracture of proximal fibula, who underwent conservative treatment with analgesics and partial weight bearing with 2 crutches. Patient have good clinical course with complete consolidation of the fracture at 3 months, but pain and increased volume persisted in the anterior aspect of the leg. Local examination revealed no obvious swelling in the leg at rest, with patient lying in the supine position, also no evidence of any sensorineural deficit or varicose veins. An MRI of the leg is requested and is reported as normal. Patient insists that he is quite well at rest but when he stand he presents pain and also “a palpable mass”. On standing and straining the leg muscles, there was a soft, non-tender swelling, measuring approximately 2cm, seen along the anterior aspect of the leg in its mid-part standing (Fig. 1), and reduced in supine. Dynamic ultrasound was performed with a patient standing and forcing dorsiflexion of the foot, confirming herniation of the anterior tibial muscle with partial disruption of its fascia, a hernia of 11.7mm in size with a 3-cm extension (Fig. 2). Conservative treatment is carried out by our rehabilitation team with anti-inflammatory treatment (magnetotherapy)+local compression with bandages.

Patient presented good clinical evolution, at 4 months after starting the treatment he refers decreased pain and absence of hernia, which was confirmed by clinical examination and new ultrasound. Patient returns to his work activity without incident.
DiscussionMuscle hernias are focal herniations of muscle tissue through a defect in its fascial sheath. They are most commonly found in the lower extremity. They are mostly underdiagnosed or misdiagnosed as muscle hematomas and varicosities.1 There are about 200 cases of muscle hernias described in the literature. In 1929, Hugo Ihde reported a case series of 12 patients with muscle hernias along with their classification.2 Ihde divided muscle hernias into two groups: traumatic and constitutional. Constitutional or congenital hernias occur due to weakness in muscle fascia after chronic stress. It has been proposed that there are fenestrations in the muscle compartments through which perforating veins enter. Due to chronic stress, the fenestrations enlarge and eventually muscle hernias bulge through these openings.3 Traumatic or acquired hernias are seen secondary to penetrating trauma, direct trauma causing closed fracture with fascial tear and indirect trauma (force applied to contracted muscle causing fascial rupture).4 The anterolateral tibial compartment is the commonest site due to being a superficial and tight fascial compartment.5 A high index of suspicion and awareness of a muscle hernia helps in its early diagnosis. In the lower extremity, tibialis anterior muscle hernia is found most frequently due to the vulnerability of its fascia to trauma. The other muscles affected in the lower extremity are extensor digitorum longus, peroneus longus, peroneus brevis and gastrocnemius.6 In our case, there was a history of blunt trauma to the leg 4 years before that might have contributed to muscle hernia. On clinical examination, muscle hernia may present as a palpable bulge, soft tissue mass or subcutaneous nodule. The muscle typically herniates during leg dorsiflexion, also known as “fencer's lunge” position.7 The swelling reduces when the patient is supine or the muscle is relaxed. Although the clinical picture points towards the diagnosis, imaging, especially ultrasound, should be used to confirm it. The differential diagnosis of muscle hernias includes varicosities, angiomas, arteriovenous malformation, lipomas, ruptured muscle (a pseudohernia) and soft tissue tumours.4 However, these tumours do not show movement on changing the patient position. Dynamic sonography is diagnostic in detecting a myofascial defect and can confirm the diagnosis. Dynamic sonography can detect a muscle bulge through the fascial defect on muscle contraction and its retraction on relaxation. Sonography is advantageous as it is a real-time modality, so that muscle herniation is detected during a dynamic examination, and the nature of lesion can be shown to the patient, which is reassuring. The examination is done in a standing position or by contracting the muscle.8 A 3D scan allows for a better delineation of fascial defects with a proper placement of the reference point. A 3D scan highlights the muscle herniation and makes hernia easy to see.9 MRI is useful in equivocal USG findings and confirms muscle herniations with a better musculofascial demarcation.10 There is no ideal treatment for muscle herniations described in the literature. Most hernias are asymptomatic and require only reassurance. Mildly symptomatic hernias are treated conservatively with rest, restriction of exercise and the use of compression stockings. Various surgical techniques for symptomatic hernias include decompressive fasciotomy, primary fascial repair – including direct closure of the defect, closure of the defect using autologous or synthetic grafts, etc.11
ConclusionsTibialis anterior muscle hernia is a rare diagnosis and should be considered in the differential diagnosis in a patient with chronic leg pain and swelling. Dynamic ultrasound is crucial in confirming the diagnosis and should be done on straining the muscles of the affected limb.
Conflict of interestThe authors declare that they don’t have any conflict of interests.

