






There is an increase in the number of participants in long distance races as well as the interest in knowing their effects on health. Our main objective is to analyse the characteristics of mountain marathon runner, its effects on health and whether there are differences between elite and non-elite runners.
MethodsThe Serialmed-UP is a pilot, observational (cohort) prospective study carried out at the Ultra Pirineu Marathon 2017. A survey of health, nutrition and training habits was carried out among non-élite runners. Clinical and analytical variables were measured before and after the race. A descriptive and comparative study was performed between results before and after the race and among élite and non-élite runners.
Results29 runners participated in the study, 22 non-élite and 7 élite. The non-élite were mostly men with a median age of 39 years-old, with good cardiovascular health (90.9% with recent medical check-ups), with a high load of training (professional counselling in 72.7%) and good eating habits (counselling in 54.5%). Before the race, there were no clinical or analytical alterations but 33.3% had alterations in the ECG. The most notable findings after the race were weight loss (3% of body weight), acute renal failure (66.7%) and alterations in sodium (44%), being these alterations more significant in non-élite runners.
ConclusionsLong distance races have an impact on runners’ health, especially among non-élite runners. We need more research in order to offer personalised recommendations based on scientific evidence.
Incremento del número de participantes en carreras de larga distancia, así como el interés por conocer sus efectos sobre la salud. El objetivo principal es analizar las características de los corredores de una maratón de montaña, sus efectos sobre la salud y si existen diferencias entre los corredores de élite y de no élite.
MétodosEl estudio Serialmed-UP es un estudio piloto, observacional, de cohortes prospectivo que se realizó en la Maratón Ultra Pirineu 2017. Se realizó una encuesta sobre hábitos de salud, alimentarios y de entrenamiento a los corredores de no élite. Se midieron las variables clínicas y analíticas antes y después de la carrera. Se realizó un estudio descriptivo y comparativo entre resultados antes y después de la carrera entre corredores de élite y de no élite.
ResultadosParticiparon 29 corredores, 22 de no élite y 7 de élite. Los de no élite son principalmente varones de mediana edad de 39 años, con buena salud cardiovascular (el 90,9% con revisiones médicas recientes), con alta carga de entrenamientos (asesoramiento profesional en el 72,7%) y buenos hábitos alimentarios (asesoramiento en el 54,5%). Antes de la carrera no había alteraciones clínicas ni analíticas, pero el 33,3% presentaban alteraciones en el ECG. Los hallazgos más destacables post-carrera fueron pérdida de peso (3% del peso corporal), insuficiencia renal aguda (66,7%) y alteraciones en el sodio (44%), fueron más significativos en los corredores de no élite.
ConclusionesLas carreras de larga distancia tienen repercusión en la salud de los corredores, sobre todo en los de no élite. Es necesario realizar más investigaciones para poder aportar recomendaciones personalizadas basadas en la evidencia científica.
The prescription of physical exercise to prevent cardiovascular and non-cardiovascular mortality has been proven to be useful. Moderate aerobic exercise for a minimum of 30min, 5 days a week, or vigorous exercise for 20min, 3 days a week, is recommended to achieve these benefits. Physical exercise can also entail injury and risk but, overall, the benefits outweigh the risks.1
Recent years have seen an increase in the number of people who run, and they are currently undertaking long distances such as marathons and ultramarathons. In many cases, the amount and intensity of training and competitions far outweigh the recommendations for maintaining good health.2 In parallel, there is some concern as to the constraints that exercising entail and whether they are the same for everyone.3 Therefore there is increased interest in exploring the effects of high duration and intensity exercise on health, and whether there is an upper limit at which the harmful effects of physical exercise might outweigh its benefits.
Serialmed-UP is a pilot study with the principal aim of analysing the characteristics of a group of mountain marathon runners, the immediate effects of the race on their health and whether there are differences between elite and non-elite runners. The secondary aim is to explore whether implementing ongoing health measures is helpful in improving runners’ awareness and preparedness in order to prevent risks to their health in the future.
Material and methodsDesign and scope of the studySerialmed-UP is an observational cohort prospective study. The main objectives of the company Serialmed LAB S.L. are to research the effects of sport on health and promote healthy lifestyle habits.4 The scope of the study was the Ultra Pirineu (UP) mountain marathon that took place in the municipality of Bellver de Cerdanya on 23 September 2017. The marathon comprised a mountain run of 45km with a positive vertical drop of 2400m.5
Selection of participants and data compilationTo select participants, runners were sent an email (via the organiser), explaining the pilot study and encouraging them to take part voluntarily. The data compilation for the study was divided into two parts. First, a few weeks before the race, a survey on health, dietary and training habits was sent by email. The second part entailed clinical and analytical measurements the evening before the race (pre-race) and immediately after the finish line (post-race) within a maximum interval of 15min. The order of systematic data collection order was as follows: first, the runner was weighed on a calibrated scale (with shorts and socks and before any fluid intake), then their blood pressure (BP), heart rate and oxygen saturation seated in an armchair were taken, and finally an electrocardiogram (ECG) at rest was performed and venous blood taken with the runner lying down on a stretcher.
Study variablesThe survey sent by email in the first part of the study included the following variables: demographic, anthropometric, medical history and cardiovascular risk factors, training and dietary habits. The degree of adherence to a Mediterranean diet was assessed within the dietary habits, since it is currently considered the diet with the greatest benefits in terms of primary cardiovascular disease prevention. The Predimed test was used. This is a validated instrument comprising a set of 14 short questions scored between 0 and 14 points and classifying the degree of adherence as low (<7 points), intermediate (7–10 points) or high (10–14 points).6
The variables collected in the second part of the study (before and after the race) were as follows: clinical variables (weight, BP, heart rate and oxygen saturation), ECG at rest and blood test variables (haemoglobin, haematocrit, venous blood gas, blood sugar, creatinine, lactate, sodium, potassium, ionic calcium and chlorine). The “epoc Host2®” system from Alere™ was used for the blood analyses, which enables immediate results without the need to process and transport blood samples.7 Any increase in serum creatinine of 0.3mg/dl or above (or an increase of 50% or above of baseline) between the level before and after the race was considered acute kidney failure.8
All the volunteers who participated in the study read and signed their informed consent before any tests were performed.
Statistical methodologyThe Shapiro–Wilks test was used to determine whether the quantitative variables followed a normal distribution. The quantitative variables were expressed in medians and interquartile range, and the qualitative variables as numbers and percentages. Pearson's χ2 test was used to compare the qualitative variables. The Student's t-test was used to compare the quantitative variables for independent samples, and the Student's t-test for paired samples to compare the quantitative variables before and after the race. Non-parametric tests were used such as the Mann–Whitney U test to perform these comparisons in the event of distribution that was not normal. A p value below .05 was considered statistically significant.
ResultsA total of 29 runners took part in the Serialmed-UP study, 22 non-elite and 7 elite. Twenty-two non-elite runners took part in the first part of the study (survey), and 18 non-elite runners and 7 elite runners took part in the second part of the study (measurements before and after the race). It was possible to obtain blood samples from 9 runners, 6 non-elite and 3 elite.
Table 1 shows the results of the first part of the study in detail with the characteristics of the non-elite runners. In summary, more males participated in the study, with a mean age of almost 40 and in good cardiovascular health, of whom 4.5% were active smokers and 36.4% ex-smokers. Most of the participants had undergone a medical check and complementary examinations within the two previous years. With regard to training, most had exercised for years, trained for many days each week and frequently had professional counselling. The training disciplines were varied, running being the most common. Finally, with regard to dietary habits, more than 50% had professional counselling and adherence to a Mediterranean diet was intermediate or high in a high proportion of the runners.
Descriptive results of the survey conducted on non-elite runners.
| Variablea | |
| Number of participants | 22 |
| Demographic data | |
| Males | 18 (81.8%) |
| Age (years) | 39.2 (7.9) |
| Height (m) | 1.7 (0.1) |
| Smoking | |
| Active smoker | 1 (4.5%) |
| Ex-smoker | 8 (36.4%) |
| Never smoked | 13 (59.1%) |
| Cardiovascular risk factors | |
| High blood pressure | 1 (4.5%) |
| Diabetes mellitus | 0 (0%) |
| Hypercholesterolaemia | 1 (4.5%) |
| Family history of cardiovascular disease | 7 (31.8%) |
| Medical check | |
| In the past two years | 20 (90.9%) |
| Electrocardiogram | 19 (86.4%) |
| Stress test | 19 (86.4%) |
| Echocardiogram | 9 (40.9%) |
| Spirometry | 9 (40.9%) |
| Blood test | 13 (59.1%) |
| Training | |
| Exercising for more than 10 years | 13 (59.1%) |
| Exercising for between 2 and 10 years | 9 (40.9%) |
| Exercising for days each week | 5.5 (1.0) |
| Exercising for hours each week | 12.0 (7.2) |
| Professional advice | 16 (72.7%) |
| Sports | |
| Swimming | 5 (22.7%) |
| Running | 20 (90.9%) |
| Cycling | 12 (54.5%) |
| Triathlon | 2 (9.1%) |
| Gym | 9 (40.9%) |
| Football, handball or basketball | 3 (13.6%) |
| Tennis or paddle tennis | 3 (13.6%) |
| Diet | |
| Dietary advice | 12 (54.5%) |
| Dietary supplements | 14 (63.6%) |
| Fluid intake during training (water/isotonic drinks) | 9 (40.9%)/13 (59.1%) |
| Adherence to Mediterranean diet (score)b | 9.0 (2.0) |
| Adherence: low/intermediate/highb | 1 (4.5%)/18 (81.8%)/3 (13.6%) |
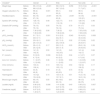
Table 2 describes the results of the measurements before and after the race, and the comparison between the elite and the non-elite runners. Overall, we can see that there were no significant alterations in the clinical variables and analyses before the race. The most relevant alterations were as follows: a third of the participants had some alteration on the ECG before the race (in particular incomplete right branch block (IRBB) of the bundle of His, 4 cases (44%) had sodium alterations after the race (particularly hypernatraemia) and almost two thirds had signs of acute kidney failure. Furthermore, it was observed that most of the runners lost weight during the race - close to 3% of their body weight. We found some differences when we compared these results between the elite and the non-elite runners (not all of them statistically significant): the elite runners were younger, finished the race in a faster time, weighed less and lost less weight during the race. In terms of vital signs, the elite runners had higher levels of saturation and lower BP and heart rate compared to the non-elite runners, and the elite runners had a higher proportion of IRBB on the ECG. Some differences were found on the blood analyses as well (not all statistically significant): the elite runners had higher baseline lactate levels, and lower ionic calcium, haemoglobin, haematocrit and blood sugar levels.
Descriptive results of the measurements before and after the race and comparative results between the elite and the non-elite runners.
| Variablesa | Total | Élite | No élite | p |
|---|---|---|---|---|
| Number | 25 | 7 (28%) | 18 (72%) | |
| Demographic data | ||||
| Males | 21 (84%) | 5 (71.4%) | 16 (88.9%) | 0.29 |
| Age (years) | 37.3 (12.2) | 30.8 (15.2) | 37.5 (9.6) | 0.23 |
| Race times | ||||
| Finisher | 23 (92%) | 6 (85.4%) | 17 (94.4%) | 0.47 |
| Race time (hours) | 6.2 (2.1) | 4.6 (1.5) | 6.3 (1.3) | <0.001 |
| Speed (km/h) | 7.3 (2.5) | 10.9 (2.8) | 7.1 (1.5) | <0.001 |
| Weight N=19 | ||||
| Weight before the race (kg) | 69.4 (14.2) | 60.0 (16.0) | 72.0 (12.7) | 0.001 |
| Weight after the race (kg) | 66.9 (12.8) | 56.7 (12.6) | 71.7 (8.7) | 0.001 |
| Difference in weight (kg) | −1.9 (1.4) | −1.5 (1.8) | −2.1 (1.5) | 0.32 |
| Weight loss | 17 (89%) | 5 (83.3%) | 12 (92.3%) | 0.55 |
| % of weight loss | −2.8 (1.9) | −2.7 (3.3) | −3.0 (1.9) | 0.78 |
| Vital signs | ||||
| Oxygen saturation (%) before the race | 98 (2) | 99 (1) | 98 (1) | 0.003 |
| Oxygen saturation (%) after the race | 96 (4) | 95 (5) | 96 (4) | 0.37 |
| Heartbeat (bpm) before the race | 64 (16) | 58 (10) | 72 (16) | 0.05 |
| Heartbeat (bpm) after the race | 97 (19) | 93 (8) | 103 (21) | 0.25 |
| Systolic BP (mmHg) before the race | 128 (10) | 122 (17) | 128 (14) | 0.02 |
| Systolic BP (mmHg) after the race | 110 (15) | 116 (16) | 110 (22) | 1.00 |
| Diastolic BP (mmHg) before the race | 79 (13) | 74 (12) | 81 (17) | 0.44 |
| Diastolic BP (mmHg) after the race | 75 (12) | 76 (14) | 75 (14) | 0.64 |
| Electrocardiogram N=21 | ||||
| Normal | 14 (66.7%) | 3 (42.9%) | 11 (78.6%) | 0.11 |
| Incomplete right branch block | 6 (28.6%) | 4 (57.1%) | 2 (14.3%) | |
| Ventricular overload | 1 (4.8%) | 0 (0%) | 1 (7.1%) | |
| Blood test N=9 | ||||
| pH before the race | 7.36 (0.02) | 7.36 (0.03) | 7.36 (0.03) | 1.00 |
| pH after the race | 7.38 (0.03) | 7.38 (0.03) | 7.38 (0.03) | 0.50 |
| pCO2 before the race (mmHg) | 51.7 (5.1) | 51.6 (2.5) | 52.4 (6.3) | 0.79 |
| pCO2 after the race (mmHg) | 40.6 (7.1) | 44.2 (5.1) | 40.4 (5.6) | 0.74 |
| pO2 before the race (mmHg) | 25.6 (6.1) | 22.7 (1.6) | 27.5 (6.8) | 0.18 |
| pO2 after the race (mmHg) | 25.4 (14.3) | 25.2 (16.9) | 25.8 (9.7) | 0.61 |
| HCO3 before the race (mmol/L) | 29.4 (1.0) | 29.2 (1.2) | 29.6 (1.6) | 0.13 |
| HCO3 after the race (mmol/L) | 25.3 (2.9) | 26.5 (1.5) | 24.8 (6.5) | 0.55 |
| Na+ before the race (mmol/L) | 141 (2) | 141 (0) | 141 (4) | 0.41 |
| Na+ after the race (mmol/L) | 142 (6) | 142 (4.5) | 142 (7) | 0.75 |
| Hyponatraemia after the race | 1 (11%) | 0 (0%) | 1 (16.7%) | 0.45 |
| Hypernatraemia after the race | 3 (33%) | 1 (33.3%) | 2 (33.3%) | 1.00 |
| K+ before the race (mmol/L) | 3.9 (0.6) | 3.8 (0.2) | 4.1 (0.7) | 0.51 |
| K+ after the race (mmol/L) | 4.7 (0.4) | 4.6 (0.2) | 4.7 (0.6) | 0.95 |
| Ca+ before the race (mmol/L) | 1.1 (0.07) | 1.1 (0.03) | 1.2 (0.05) | 0.005 |
| Ca+ after the race (mmol/L) | 1.2 (0.06) | 1.1 (0.02) | 1.2 (0.07) | 0.035 |
| Chlorine before the race (mmol/L) | 103 (4) | 105 (1.5) | 102 (4) | 0.15 |
| Chlorine after the race (mmol/L) | 106 (4) | 105 (1.5) | 106 (5) | 0.81 |
| Haematocrit before the race | 44 (6) | 41 (4) | 44 (5) | 0.36 |
| Haematocrit after the race | 46 (8) | 40 (6.5) | 47 (5) | 0.38 |
| Haemoglobin before the race | 14.9 (2.0) | 13.8 (1.4) | 15.2 (1.6) | 0.27 |
| Haemoglobin after the race | 15.6 (2.8) | 13.7 (2.1) | 16.0 (1.9) | 0.39 |
| Blood sugar before the race (mg/dl) | 95 (14) | 85 (16.5) | 96 (13) | 0.06 |
| Blood sugar after the race (mg/dl) | 90 (49) | 90 (13) | 89 (75) | 0.63 |
| Lactate before the race (mg/dl) | 0.9 (0.6) | 1.4 (0.28) | 0.9 (0.3) | 0.04 |
| Lactate after the race (mg/dl) | 2.6 (0.7) | 2.3 (0.72) | 2.7 (1.0) | 0.22 |
| Creatinine before the race (mg/dl) | 0.9 (0.3) | 0.8 (0.1) | 0.9 (0.3) | 0.13 |
| Creatinine after the race (mg/dl) | 1.5 (0.6) | 1.2 (0.6) | 1.6 (0.8) | 0.39 |
| Acute renal failureb | 6 (66.7%) | 2 (66.7%) | 4 (66.7%) | 1.00 |
The quantitative variables are presented as medians and interquartile range and the qualitative variables as numbers and percentages.
Acute renal failure is defined as an increase in serum creatinine of 0.3mg/dl or more (or an increase of 50% or more of its baseline level) between the level before and after the race.
Abbreviations: BP: blood pressure; pCO2: partial pressure of carbon dioxide; pO2: partial pressure of oxygen; HCO3: bicarbonate; Na+: sodium; K+: potassium; Ca+: calcium
When we compared the results before and after the race (Table 3), we observed that all the runners had significant weight loss, decreased oxygen saturation and increased heart rate. We also observed some essential changes in the blood analyses; the most significant were increases in potassium, lactate and creatinine. There were also increases in haemoglobin and haematocrit, which were not statistically significant. When the differences before and after the race were analysed stratifying the result into elite and non-elite runners, some relevant differences were also observed. Thus, the weight loss and rise in lactate and creatinine were only statistically significant in the non-elite runners. In contrast, the increased potassium after the race was only significant in the elite runners.
Comparative results of measurements before and after the race.
| Variablea | Overall | p | Elite | p | Non-elite | p | |
|---|---|---|---|---|---|---|---|
| Weight (kg) | Before | 69.4 (13.2) | <0.001 | 58.3 (12.5) | 0.056 | 72.5 (10.2) | <0.001 |
| After | 66.9 (12.8) | 56.7 (12.6) | 71.7 (8.7) | ||||
| Oxygen saturation (%) | Before | 98 (2) | 0.001 | 99 (1) | 0.02 | 98 (1) | 0.02 |
| After | 96 (4) | 95 (5) | 96 (4) | ||||
| Heartbeat (bpm) | Before | 64 (16) | <0.001 | 58 (10) | <0.001 | 72 (16) | <0.001 |
| After | 97 (19) | 93 (8) | 103 (21) | ||||
| Systolic BP (mmHg) | Before | 128 (10) | 0.48 | 122 (17) | 0.15 | 128 (14) | 0.46 |
| After | 110 (15) | 116 (16) | 110 (22) | ||||
| Diastolic BP (mmHg) | Before | 79 (13) | 0.05 | 74 (12) | 0.79 | 81 (17) | 0.03 |
| After | 75 (12) | 76 (14) | 75 (14) | ||||
| pH | Before | 7.36 (0.02) | 0.06 | 7.36 (0) | 0.21 | 7.35 (0.03) | 0.25 |
| After | 7.38 (0.03) | 7.38 (0.03) | 7.38 (0.03) | ||||
| pCO2 (mmHg) | Before | 51.7 (5.1) | 0.001 | 51.6 (2.5) | 0.043 | 52.4 (6.3) | 0.008 |
| After | 40.6 (7.1) | 44.2 (5.1) | 40.4 (5.6) | ||||
| pO2 (mmHg) | Before | 25.6 (6.1) | 0.001 | 22.7 (1.6) | 0.02 | 27.5 (6.8) | 0.02 |
| After | 25.4 (14.3) | 25.2 (16.9) | 25.8 (9.7) | ||||
| HCO3 (mmol/L) | Before | 29.4 (1.0) | 0.17 | 29.2 (1.2) | 0.03 | 29.6 (1.6) | 0.38 |
| After | 25.3 (2.9) | 26.5 (1.4) | 24.8 (6.5) | ||||
| Na+ (mmol/L) | Before | 141 (2) | 0.50 | 141 (0) | 0.43 | 141 (4) | 0.84 |
| After | 142 (6) | 142 (4.5) | 142 (7) | ||||
| K+ (mmol/L) | Before | 3.9 (0.6) | 0.006 | 3.8 (0.2) | 0.04 | 4.1 (0.7) | 0.07 |
| After | 4.7 (0.4) | 4.6 (0.2) | 4.7 (0.6) | ||||
| Ionic Ca+ (mmol/L) | Before | 1.1 (0.07) | 0.36 | 1.1 (0.03) | 0.59 | 1.2 (0.05) | 0.56 |
| After | 1.2 (0.06) | 1.1 (0.03) | 1.2 (0.07) | ||||
| Chlor (mmol/L) | Before | 103 (4) | 0.13 | 105 (1.4) | 0.53 | 102 (4) | 0.17 |
| After | 106 (4) | 105 (1.5) | 106 (5) | ||||
| Haematocrit | Before | 44 (6) | 0.18 | 41 (4) | 0.73 | 44 (5) | 0.21 |
| After | 46 (8) | 40 (6.5) | 47 (5) | ||||
| Haemoglobin | Before | 14.9 (2) | 0.14 | 13.8 (1.4) | 0.51 | 15.2 (1.6) | 0.23 |
| After | 15.6 (2.8) | 13.7 (2.1) | 16.0 (1.9) | ||||
| Blood sugar (mg/dl) | Before | 95 (14) | 0.55 | 85 (16.5) | 0.41 | 96 (13) | 0.75 |
| After | 90 (49) | 90 (13) | 89 (75) | ||||
| Lactate (mg/dl) | Before | 0.96 (0.6) | 0.006 | 1.41 (0.28) | 0.40 | 0.90 (0.3) | 0.007 |
| After | 2.58 (0.7) | 2.27 (0.72) | 2.69 (0.9) | ||||
| Creatinine (mg/dl) | Before | 0.97 (0.3) | 0.013 | 0.83 (0.09) | 0.20 | 0.98 (0.3) | 0.05 |
| After | 1.49 (0.7) | 1.23 (0.57) | 1.58 (0.7) |
Serialmed-UP is a pilot study that included 29 mountain marathon runners, which enabled us to study, on the one hand, their health, training and nutrition habits and, on the other, any immediate alterations to their health, and finally we were able to examine whether there were any differences between the elite and the non-elite athletes.
The non-elite runners were around 40 years of age, and overall, had better health, and good dietary and training habits. They showed no alterations in the baseline variables analysed on the day before the race. This is positive and should be maintained for all non-elite runners wishing to take part in a mountain marathon. It is likely that these results cannot be applied to other non-elite runners. It is possible that the fact that participation in the study was voluntary enabled the selection of individuals who were more concerned about their health and consequently had better habits. It would be useful to analyse a greater number of non-elite runners (chosen randomly and not on a voluntary basis) to determine whether the same results are reproduced.
The fact that the great majority of the participants had undergone a medical check-up within the previous two years9 highlights their awareness of sports safety and might encourage sports’ test organisers to recommend or even demand certificates of fitness in order to participate in competitive events.
A high proportion (near 30%) of the sportspeople showed IRBB on their ECG in the baseline tests before the race, and was more common in the elite runners than the non-elite runners. Complete right branch block is an electrocardiographic alteration that presents above all in older individuals (over 50 years of age) and is rare in those aged under 30 (estimated prevalence of 0.2%).10 By contrast, IRBB is a more frequent finding in healthy and younger individuals, with estimations of prevalence of up to 13.5% in some studies.11 IRBB in athletes has been described frequently (between 9% and 24% according to the series) and together with early repolarisation and sinus bradycardia, is considered a benign disorder and a marker of physiological and structural adaptation to intense physical exercise.12–14
With regard to weight, almost 90% of the participants had lost some weight after the race, this was more frequent in the non-elite runners, even when this difference was not statistically significant. Almost 3% of body weight was lost and was also more frequent in the non-elite runners. Dehydration (loss greater than 2% of body weight as water) might degrade the performance of aerobic exercise, especially in hot environments. The greater the dehydration, the higher the physiological effort and the poorer the performance during aerobic exercise. A reduction in total available body water results in a reduction of total volume, systolic volume and cardiac output.15 Dehydration (whether hypo, hyper or isotonic) can entail symptoms after a 1% loss of body weight (malaise, muscle weakness, etc.) and can even result in death if it increases to around 8%-10%. Thirst is not a completely reliable indicator of dehydration, since it occurs when weight loss has reached 1%–3%, therefore runners should be aware of this fact and drink even if they are not thirsty during the race.16
A large proportion of runners showed altered kidney function and electrolytes after the race, two thirds showed elevation of creatinine with signs of acute kidney failure and 44% altered sodium, particularly hypernatraemia. These alterations are common and well described in the literature; it has been suggested that they are occasionally present before starting the competition.17 None of the participants in this study had altered renal function or natraemia the day before the race, which indicates that these alterations directly relate to physical exercise. Normally this renal dysfunction is pre-renal in nature and secondary to volume depletion due to suboptimal hydration. The increased haemoglobin levels after the race (although not statistically significant) as a measure of haemoconcentration would confirm this hypothesis. Even so, the possibility of kidney failure in the absence of volume depletion has been described, and it has been posited that strenuous physical exercise may result in systemic disorders, including an inflammatory condition that per se might cause damage to the nephrons.18 Many of the biochemical alterations that have been described in relation to physical exercise are asymptomatic and transitory, but it is not known whether they might have a harmful effect on health in the long term.19–22 It would be desirable to know the recovery time of post-race alterations and be able to make recommendations as to when training and/or competing can be resumed.
It is important to observe how most of the differences between the levels before and after the race were only statistically significant in the non-elite runners, the weight loss, increased creatinine and increased lactate being noteworthy even when the baseline lactate levels (before the race) were higher in the elite runners. Blood lactate levels are a marker of the intensity of exercise,23 and it is possible that the musculature of elite runners is better adapted to running and that they have far more developed lactate clearance, which might explain why their lactate increase after the race was lower than that of the non-elite runners.
We also observed a drop in blood sugar and haemoconcentration (increased haemoglobin and haematocrit) in the non-elite runners, although neither finding was statistically significant. Thus, the non-elite runners, despite apparently retaining their baseline characteristics (health status, training and diet), had more alterations after the race than the elite runners. It is likely that their level of training, diet and rest, and the fact that they required far longer to complete the race than the elite runners contributed, in part, to these findings.
The results of the Serialmed-UP study enable us to examine the practical applicability of a work model that combines assistance and research. Assistance would imply an analysis of the health and training habits of the athlete, with the potential to make immediate recommendations. Research through obtaining, accumulating and analysing data on the effects of endurance training on health, would enable us to make recommendations to athletes (both elite and non-elite) based on scientific evidence. A subjective yet positive perception of this study (by runners and researchers alike) was that the results were available immediately, which in turn enabled immediate recommendations. Significant alterations in the clinical and/or analytical parameters detected before the race would make it necessary to advise against taking part in the competition. Detecting alterations in the evaluations made after the race (as occurred in the study) enabled us to make recommendations in situ to be implemented over the following days (rest, hydration, repeat the tests in a few days, improved diet or training, etc.) and for future competitions (improving hydration while racing, for example).
We are aware that the Serialmed-UP study has limitations. Firstly, the size of the sample studied was small and does not enable the findings to be generalised. It is also likely that it did not enable more statistically significant differences to be demonstrated when comparing some variables, when in reality this should be the case. Furthermore, the participants were selected on a voluntary not a random basis from all the runners in the race, and this probably led to some selection bias. It is likely that those who decided to participate voluntarily in the study had different characteristics (motivation and habits) to those who did not wish to take part.
In conclusion, given the increased number of non-elite participants in long distance and endurance races, knowledge of the potential effects on health must be advanced, in order to offer recommendations based on scientific evidence.
Conflict of interestsAuthors declare that they don’t have any conflict of interests.
We would like to thank the organisers of Ultra Pirineu for providing every facility to undertake this study, and all the runners who took part voluntarily.

