





In periods of confinement, people cannot be assessed in training centers. Therefore, it is essential to have valid and reliable tests to evaluate physical capacities remotely and with their respective valuation tables.
ObjectiveTo determine the validity and reliability of the Muscular Fitness Test (MFT) to evaluate the body strength-resistance with self-loading in healthy young adults. Secondly, to create qualitative scales to evaluate the different levels of this physical capacity.
Material and methods489 participants performed the MFT (test), and 77 performed it twice (re-test). The MFT included 60seconds (s) of sit-ups, push-ups, deep squats, and burpees, always in that order, with a micropause of 10s. The validity of the MFT was evaluated with the final heart rate (FHR), % of the reserve HR (%) and Rating of Perceived Exertion (RPE); the reliability included the Coefficient of Variation (CV), Intra-Class Correlation Coefficient (ICC) and the standard error of the mean (SEM) (p<0.05). The qualitative scales were constructed with the percentiles ≤25: poor, ≤50: fair, ≤75: good, ≤90: very good, and >90: excellent.
ResultsParticipants performed 91.7±26.5 total repetitions, with a FHR of 172.7bpm (81.7%) and RPE of 8.1; CV=2.81%, ICC=0.97 and SEM=0.77 (p<0.001).
ConclusionMFT proved to be valid and reliable to assess self-loaded body strength-resistance in healthy young adults. The creation of the MFT qualitative scales allows evaluating the level of body strength-resistance in this population.
Strength training and development is considered an essential component for the increase of the population's physical condition1 and essential for delivering support and maintenance of body posture.2 It is a fact that the daily movements that people exercise need strength, and that some of these physical efforts are sustained over an extended period3; for these last efforts, strength-resistance (S-R) plays a fundamental role. S-R is defined as the capacity that a muscle group possesses to maintain repeated contractions against a load (resistance) during a prolonged period.4 This physical capacity has become an important agent within the physical condition and should be taken into account when evaluating the musculoskeletal functions5 and the physical capacities of the population.6
There are a large number of tests to evaluate physical abilities.7 Some of these tests are carried out in laboratories8 and others directly in the field.6 The most used field tests to evaluate the physical condition are sit-ups, push-ups, deep squats, and burpees, among others; however, it is essential to mention that, for evaluating S-R of both upper and lower extremities, these tests must be performed until exhaustion.9 Although these tests evaluate specific muscle groups, there are several execution protocols in the sports field; within these variations we can mention the execution time, the joint ranges, and the evaluation planes.10,11
Physical tests measuring S-R in different muscle groups have been independently validated in different populations.6,12,13 Thus, the tests for abdominal muscles, elbow, hip, and knee flexo-extensors, which allow predicting the performance of both muscle strength and S-R,14 have been validated in an isolated way and not as a whole.6,14 In this sense, some studies have reported a good association between the flexo-extension test of elbows and the press-bench test of a maximum repetition (1RM).15 Also, some investigations have concluded that an adequate level of S-R, evaluated through the flexo-extension test of elbows, is associated with better metabolic health.16 On the other hand, it has been shown that an increase in the Body Mass Index (BMI) has a negative influence on S-R levels.14,17 However, as far as knowledge goes, a test's validity and reliability to measure S-R with four consecutive and continuous exercises in healthy adults from 18 to 25 years old have not been determined.
On the other hand, and as a result of the pandemic generated by the COVID-19, government authorities worldwide have implemented stringent health measures for the population. Among the first measures is the isolation of symptomatic patients; however, as the days go by, other measures have been developed, such as the prohibition of mass gatherings, the mandatory closure of educational establishments, and even confinement in private homes for unspecified periods.18 Confinement measures, which are intended to prevent the spread of the virus, could negatively affect the population.19 Thus, it has been observed that this confinement generates a lower level of physical activity and more significant sedentary behavior.20 This condition can cause a decrease in the quality of life of the people.21
As a result of the confinement, a large part of the population has not been able to access physical training centers (gyms, clubs, sports schools) nor develop the physical exercise routines correctly; similarly, competitive athletes have not been able to attend the high-performance centers or the laboratories to develop and evaluate the different parameters of the physical condition.19 For this reason, in this period of confinement, it is essential to have valid and reliable tests to evaluate physical condition parameters. Currently, there is no test to evaluate S-R with four consecutive and continuous self-loading exercises at low cost and with qualitative scales indicating different levels of S-R for both men and women.1 Consequently, this study's primary purpose was to determine the validity and reliability of the Muscular Fitness Test (MFT) to evaluate self-loading body strength-resistance in healthy and physically active young adults from 18 to 25 years old. As a secondary objective, the MFT qualitative scales were created to evaluate the different levels of body S-R in men and women.
Material and methodsResearch designResearch with a quantitative focus, exploratory-descriptive scope, non-experimental design of the predictive cross-sectional type.22 To determine the validity and reliability of the MFT, five sessions separated by 48h were executed: session 1) briefing, informed consent acceptance (google.docs®) and anthropometric assessment; sessions 2 and 3) familiarization with exercises and MFT; session 4) first application of MFT, and session 5) second application of MFT (Fig. 1a).
Procedures Research design. (b) Muscular Fitness Test: exercises and sequence.")
As a first action, all participants who voluntarily accepted to participate in the study (non-probabilistic sample) were invited and gathered to be informed. In the informative talk, the purpose and procedures of the study were clarified. The inclusion criteria were that all participants should be healthy, physically active23 and between 18 and 25 years old, while the exclusion criteria were: positive COVID-19 diagnosis, the prevalence of musculoskeletal injuries, pre-existing cardiac pathologies, abnormal respiratory and cardiac responses during the familiarization period and inability to perform MFT. All participants were asked to refrain from physical activities that generate nervous or musculoskeletal fatigue 48h before the measurements and to refrain from caffeine or any substance that could increase their metabolism during the assessment. Finally, only those participants who accepted informed consent were subjected to MFT. All sessions were conducted virtually and synchronously with participants through the Zoom® platform.
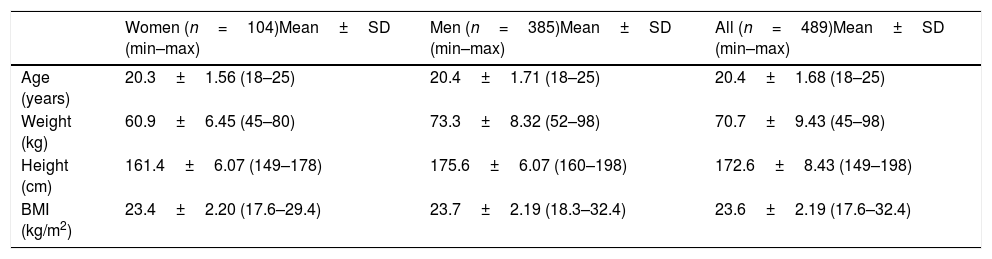
ParticipantsFour hundred eighty-nine (489) healthy and physically active young adults volunteered to participate in this study (Table 1). The type of sampling was non-probability for convenience. All participants were informed of the study objective and possible risks of the experiment. Also, all participants accepted informed consent before the application of the protocols. The informed consent and the study were approved by the Human Research Committee of the University of Las Americas (registry number CEC-FP-2020011). They were conducted under the Declaration of Helsinki (WMA 2000, Bošnjak 2001, Tyebkhan 2003), which establishes the fundamental ethical principles for research with human beings.
Characterization of the participants.
| Women (n=104)Mean±SD (min–max) | Men (n=385)Mean±SD (min–max) | All (n=489)Mean±SD (min–max) | |
|---|---|---|---|
| Age (years) | 20.3±1.56 (18–25) | 20.4±1.71 (18–25) | 20.4±1.68 (18–25) |
| Weight (kg) | 60.9±6.45 (45–80) | 73.3±8.32 (52–98) | 70.7±9.43 (45–98) |
| Height (cm) | 161.4±6.07 (149–178) | 175.6±6.07 (160–198) | 172.6±8.43 (149–198) |
| BMI (kg/m2) | 23.4±2.20 (17.6–29.4) | 23.7±2.19 (18.3–32.4) | 23.6±2.19 (17.6–32.4) |
kg: kilograms; cm: centimeters; m2: square meters; SD: standard deviation; min: minimum; max: maximum.
In order to avoid physical contact, participants were asked to self-evaluate their height (cm) and weight (kg) with the following considerations: height was measured through a stadiometer from the feet to the vertex (Frankfort plane), while weight was evaluated through a digital scale, with participants barefoot, in shorts and wearing a light shirt. In case the participants did not have access to these instruments, it was considered the last personal evaluation of these variables. The BMI interpretation was performed according to the anthropometric standards for evaluation of the nutritional status.24
Standardized warm-upFor both the first and second MFT evaluations, the warm-up consisted of four minutes (min) of upper and lower extremity joint mobility (flexions, extensions, adduction, and shoulder and hip abductions, respectively), 30seconds (s) of Skipping, 30s of heels to buttocks, 30s of jumping with hip flexions, 30s of jumping with ankle flexions (stiffness), and four min of gentle stretching. After this warm-up and before running the MFT, there was a break of 5min (Fig. 1b).
Muscular fitness testThe MFT is intended to evaluate the body's S-R with self-loading. It consists of four tests that must be executed continuously and always in the following order: hip flexo-extensions (sit-ups), push-ups, deep squats, and burpees. Each one of the tests must be executed for 60s. Each participant has to perform the greatest number of repetitions during this time; between each exercise, there is a 10s micropause. This micropause is intended for the participant to adopt the following exercise (Fig. 1b).
Hip flexo-extensions (sit-ups): test that measures the S-R of the abdominal musculature. This test is executed starting from the dorsal decubitus position with both legs together and knees extended, both arms behind with elbows extended resting on the floor. At first, the participant must bend his hips and knees until he is seated with his feet on the floor, his arms embracing the knees and his forehead exceeding the knees’ line. He will then return to the starting position lying on his back until his shoulder blades touch the floor, knees fully extended, arms behind, and elbows fully extended (Fig. 2a). Push-ups: test that measures the S-R of the elbow extensors. This test is performed starting from the abdominal position, with elbows extended and palms of the hands resting on the floor at chest level, while the trunk, thighs, and legs must be aligned throughout the execution. At first, the participant must bend the elbows symmetrically until reaching a lower angle of 90° between the arm and forearm. He will then extend his elbows to return to the starting position (Fig. 2b). Deep squats: test that measures the S-R of the extensor muscles of the knees and hips. This test is executed starting from the standing position with arms in front, elbows fully extended, and in front of the shoulders during the whole execution. To start, the participant must bend his knees and hips symmetrically until reaching an angle of less than 90° between the thighs and legs. He will then extend his knees and hips to return to the starting position (Fig. 2c). Burpees: test that measures the S-R of the abdominal musculature, back, chest, arms and legs, simultaneously and in a coordinated manner. This test is executed starting from the standing position with the arms at the side of the body. From that position, the participant descends to squatting position with the palms of the hands resting on the floor. Afterward, the participant brings both legs back to extend the knees as far as possible, keeping the elbows extended and the hands’ support parallel to the height of the shoulders. Later, he returns to the squatting position and, from there, makes a vertical jump, keeping elbows extended and arms up and over the head. Finally, he lands with his feet together and on tiptoes (Fig. 2d).
 Hip flexo-extensions (sit-ups); (b) Push-ups; (c) Deep squats; (d) Burpees.")
Heart rate: The current confinement situation meant that HR could not be evaluated with electronic devices that would ensure the reliability of the measurement. Despite this and in order to estimate the intensity of the MFT, participants were asked to evaluate the heart rate in two moments (at rest and at the end of the MFT). To estimate the resting heart rate and the final heart rate, participants were asked to count the number of heartbeats in the carotid artery by 10s (this value was multiplied by 6).25 The resting heart rate and final heart rate values were considered as resting heart rate (restHR) and final heart rate (FHR), respectively. On the other hand, to calculate the maximum heart rate (maxHR), the following formula was used: (208−[0.7×age]) beats per min (bpm).26 Thus, to calculate the term intensity associated with the reserve heart rate (resHR), the following formula was used: Final Intensity (% resHR)=([FHR−restHR]/[maxHR−restHR])×100.26
Rating of Perceived Exertion(RPE): in order to evaluate the level of demand experienced by the participants at the end of the MFT, the RPE scale (1–10) was applied.27
Statistical analysisDescriptive data are presented as means and standard deviations. The normal distribution of the data was confirmed by the Shapiro–Wilk test (p>0.05). The MFT validity was determined by relating the mean values of FHR, Final Intensity (% of resHR), RPE, and the time of execution (4min 30s). The reliability of the MFT was evaluated through the Coefficient of Variation (CV), the Intra-class Correlation Coefficient (ICC), the standard error of the mean (SEM), and the corresponding 95% confidence interval. Acceptable reliability was determined as a CV<10% and a ICC>0.85.28 The t-tests for related samples and the Bland–Altman technique were used to evaluate the concordance between the MFT test and re-test.29 For creating the qualitative scales, the percentile distribution was used with the following criteria: ≤25%: poor; ≤50%: fair; ≤75%: good; ≤90%: very good; and >90%: excellent. All other statistical analyses were performed with SPSS software version 22.0 (SPSS, Chicago, IL, USA). The significance level for all statistical analyses was p<0.05.
ResultsTo determine the validity and reliability of the MFT, 77 of the 489 participants were evaluated in two instances separated by 48h (test and re-test). The variables used to determine MFT validity were the FHR (bpm), final intensity (% of resHR) and RPE (scale 1–10). In relation to the post-exercise intensity, the analysis showed that the FHR was 172.4±22.7 and 173.1±20.6bpm for the test and re-test, respectively (CV=0.78%; ICC=0.87; SEM=1.23; p=0.57). The final intensity of the MFT was 81.5±15.5 and 82.0±14.4% of the resHR for the test and re-test, respectively (CV=1.67%; ICC=0.83; SEM=0.98; p=0.61). While the RPE was 8.06±1.29 and 8.17±1.20 for the test and re-test, respectively (CV=3.37%; ICC=0.87; SEM=0.07; p=0.15).
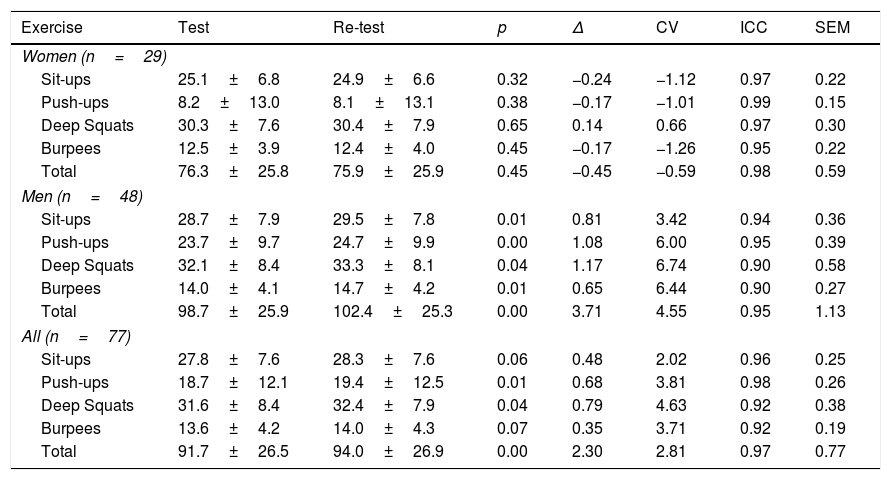
The variables used to determine the MFT reliability were the number of repetitions performed in the four exercises and the sum of all the repetitions of the MFT in both the test and the re-test. There was a maximum CV of 4.63% for the squats, while the minimum CV was 2.02% for the sit-ups. Simultaneously, the lowest ICC was 0.92 in deep squats and burpees, while the highest ICC was 0.98 in push-ups. When women were analyzed separately (29 cases), a maximum CV of −1.26% was observed for burpees, while the minimum CV was 0.59% for total MFT repetitions. In parallel, the lowest ICC was 0.95 for burpees, while the highest ICC was 0.99 for push-ups. When analyzing men separately (48 cases), a maximum CV of 6.74% was observed for deep squats, while the minimum CV was 3.42% for sit-ups; while the highest ICC was 0.95 for push-ups and the total number of repetitions in the MFT, while the lowest ICC was 0.90 for deep squats and burpees. The CVs and ICCs of all analyses are reported in Table 2 and Fig. 3.
Reliability of the Muscular Fitness Test.
| Exercise | Test | Re-test | p | Δ | CV | ICC | SEM |
|---|---|---|---|---|---|---|---|
| Women (n=29) | |||||||
| Sit-ups | 25.1±6.8 | 24.9±6.6 | 0.32 | −0.24 | −1.12 | 0.97 | 0.22 |
| Push-ups | 8.2±13.0 | 8.1±13.1 | 0.38 | −0.17 | −1.01 | 0.99 | 0.15 |
| Deep Squats | 30.3±7.6 | 30.4±7.9 | 0.65 | 0.14 | 0.66 | 0.97 | 0.30 |
| Burpees | 12.5±3.9 | 12.4±4.0 | 0.45 | −0.17 | −1.26 | 0.95 | 0.22 |
| Total | 76.3±25.8 | 75.9±25.9 | 0.45 | −0.45 | −0.59 | 0.98 | 0.59 |
| Men (n=48) | |||||||
| Sit-ups | 28.7±7.9 | 29.5±7.8 | 0.01 | 0.81 | 3.42 | 0.94 | 0.36 |
| Push-ups | 23.7±9.7 | 24.7±9.9 | 0.00 | 1.08 | 6.00 | 0.95 | 0.39 |
| Deep Squats | 32.1±8.4 | 33.3±8.1 | 0.04 | 1.17 | 6.74 | 0.90 | 0.58 |
| Burpees | 14.0±4.1 | 14.7±4.2 | 0.01 | 0.65 | 6.44 | 0.90 | 0.27 |
| Total | 98.7±25.9 | 102.4±25.3 | 0.00 | 3.71 | 4.55 | 0.95 | 1.13 |
| All (n=77) | |||||||
| Sit-ups | 27.8±7.6 | 28.3±7.6 | 0.06 | 0.48 | 2.02 | 0.96 | 0.25 |
| Push-ups | 18.7±12.1 | 19.4±12.5 | 0.01 | 0.68 | 3.81 | 0.98 | 0.26 |
| Deep Squats | 31.6±8.4 | 32.4±7.9 | 0.04 | 0.79 | 4.63 | 0.92 | 0.38 |
| Burpees | 13.6±4.2 | 14.0±4.3 | 0.07 | 0.35 | 3.71 | 0.92 | 0.19 |
| Total | 91.7±26.5 | 94.0±26.9 | 0.00 | 2.30 | 2.81 | 0.97 | 0.77 |
Δ: delta of variation; CV: coefficient of variation; ICC: intra-class correlation coefficient; SEM: standard error of measurement; p: p-value.

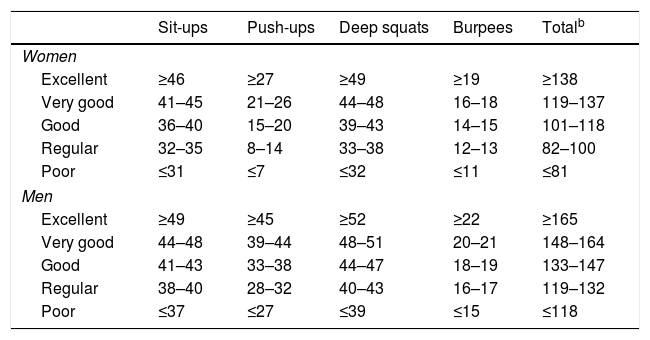
For the creation of the MFT qualitative scales, the number of repetitions made in the four exercises and the sum of all the repetitions of the MFT were used (489 cases). For the creation of these scales, the participants were evaluated in one instance (test). The different ranges and criteria are reported in Table 3.
Qualitative scale for the Muscular Fitness Test.a
| Sit-ups | Push-ups | Deep squats | Burpees | Totalb | |
|---|---|---|---|---|---|
| Women | |||||
| Excellent | ≥46 | ≥27 | ≥49 | ≥19 | ≥138 |
| Very good | 41–45 | 21–26 | 44–48 | 16–18 | 119–137 |
| Good | 36–40 | 15–20 | 39–43 | 14–15 | 101–118 |
| Regular | 32–35 | 8–14 | 33–38 | 12–13 | 82–100 |
| Poor | ≤31 | ≤7 | ≤32 | ≤11 | ≤81 |
| Men | |||||
| Excellent | ≥49 | ≥45 | ≥52 | ≥22 | ≥165 |
| Very good | 44–48 | 39–44 | 48–51 | 20–21 | 148–164 |
| Good | 41–43 | 33–38 | 44–47 | 18–19 | 133–147 |
| Regular | 38–40 | 28–32 | 40–43 | 16–17 | 119–132 |
| Poor | ≤37 | ≤27 | ≤39 | ≤15 | ≤118 |
Concerning the main objective of the study, the four variables evaluated for the determination of the validity of the MFT (time, FHR, % of the resHR and RPE), showed that the MFT is valid to evaluate the corporal S-R with self-load in young healthy and physically active adults from 18 to 25 years. Considering that the intensity of the exercise is the fundamental axis on which the metabolic predominance of the physical exercises turns,26 the convergence of the FHR (172.7bpm), the final intensity of the MFT (81.7% of the resHR), the RPE experienced by the participants (8.1 out of 10.0)27 and the duration of the MFT (4min 30s), indicate that this test allows evaluating the muscular S-R. Specifically, it evaluates the capacity of work of the muscular fibers type I and IIa in the muscles involved in the different exercises. In parallel and considering the relationship between the resHR and the consumption of reserve oxygen, the MFT could be used to evaluate the state of the mixed aerobic-anaerobic metabolism.30 However, to reliably determine the energy metabolism involved in MFT, in addition to the final intensity of the MFT, a direct assessment of oxygen consumption31 and a lactic threshold test32 should also be applied. In turn, the CV, ICC, and SEM for the four exercises and the sum of all the MFT repetitions (CV: 2.02–4.63%; ICC: 0.92–0.98; SEM: 0.19–0.77), indicate that the MFT presents a high degree of reliability.28
Before the application of MFT, and as far as knowledge goes, there were only validation studies for tests that evaluated S-R muscle groups or body segments in isolation.6,13 In this sense, the study by Bianco et al.6 examined the sit up test to evaluate muscular S-R in sedentary individuals of both sexes; in this research, upper-extremity S-R was also evaluated through push-ups and lower-extremity S-R through squats; At the end of the study and considering the low correlation coefficient between the different tests (r2=0.23; r=0.49; p<0.001 for the sit up test versus the push-up test; r2=0.31; r=0.57; p<0.001 for the sit up test versus the weighted squat test), the researchers concluded that it is not optimal to use a single test for the global evaluation of muscular S-R. In the same line, Nikolaidis et al.13 evaluated the most used methods for the election of different tests that measure muscular S-R, concluding that push-ups and squats, both timed, are the most recurrent exercises to evaluate that physical capacity. The same authors conclude that the election of a test to evaluate muscular S-R should consider the most relevant specific muscle groups associated with the specific tasks.13 Based on this background, MFT is a pioneer in the evaluation of body S-R with self-loading; besides, it is a tool that can be used by Physical Education teachers, technicians and professionals of Physical Activity and Sport, simply, remotely and synchronously (Zoom® or other digital platforms), even more in this period of confinement generated by the COVID-19.18
Concerning the secondary objective of the study, after calculating percentiles for all exercises and the sum of all MFT repetitions, for both women and men, two qualitative scales were constructed for the evaluation of body S-R with self-loading in healthy young adults from 18 to 25 years old. These scales allow us to identify the level of muscular S-R in a general way and by segments; in addition, it will allow us to monitor the advances of this physical capacity product of the physical training. About the latter, Lesinski et al.12 characterized the dose-response relationship of training associated with muscular S-R in athletes; the researchers showed a moderate effect size (ES) of this type of training on vertical jump (ES: 0.8–1.09) and a small ES on the linear velocity of specific sports (ES: 0.58–0.75). At the same time, the same researchers stated that a training period longer than 23 weeks, which includes a minimum of 6 series, 6–8 exercises and intensity between 80 and 89% with a 3–4min break are effective ways to improve muscle S-R (ES: 2.09–3.40).12
Methodological limitationsConsidering that carbohydrate metabolism is the energy pathway that mainly supports the execution of MFT (transition aerobic-anaerobic zones),26 it would be essential to evaluate post-exercise and recovery blood lactate ([La]) concentrations,32 as well as recovery HR with electronic devices. Unfortunately, given the modality of MFT execution to validate this study (through video call using the Zoom® platform), it was not possible to evaluate this variable.
ConclusionConsidering the time of execution of the MFT (4min 30s), the final intensity (% of resHR), RPE, CV, ICC, and SEM, it is concluded that the MFT is valid and reliable to evaluate the body S-R with self-loading in healthy and physically active young adults between 18 and 25 years old.
Practical applicationsFor trainers who apply the MFT, it is recommended to consider the following aspects before applying the test: (a) have a period of familiarization with the participants, (b) correct recurrent errors of execution, including the extension of body segments and execution in planes and vectors indicated for each exercise, (c) teach and use the RPE scale previously. During the MFT execution, it is recommended to consider the following aspects: (a) verbally encourage participants to perform as many repetitions as possible in each exercise, and (b) correct any poorly performed exercise. At the end of the MFT, it is suggested to consider the following: (a) evaluate the final and recovery HR with some electronic device, (b) evaluate the post-stress and recovery lactate concentrations, and (c) record the participants’ RPE.
For the interpretation of the MFT results, the qualitative scale allows evaluating the general S-R (sum of all the repetitions executed in the test) and the body segments in better or worse condition. For example, a participant may have a “very good” general S-R, but the S-R of the elbows’ flexo-extensor muscles may be “poor.” This last aspect could indicate the guidelines for a possible physical training program oriented to the muscular S-R.
Future studiesFuture studies that consider the application of MFT should include evaluation of post-effort [La] (32), an evaluation of VO2max in the laboratory for participants (31), FHR, and recovery HR with electronic devices. In this way, the doubt of the predominant metabolism during the test execution and the ventilatory implication in the results will be cleared up.
Conflict of interestThe authors declare no conflict of interest.
To the 489 participants who volunteered to be part of the study.

