




The main objective of this study was to analyze more effective muscle work on some explosive strength performance variables. The secondary objectives were to determine how gender influences results and influence of the muscle work type on physiological parameters.
Material and methodRandomized controlled trial single-blind clinical trial, allocated by blocks and by sex.
The study sample consisted of 80 healthy and active subjects divided into four muscle work groups: concentric, eccentric, concentric-eccentric and isometric.
4 sets of 12 repetitions, 1-min rest between series, were performed for dynamic workgroups. For the isometric work 6s with 20 rest. 12-min time in 12 consecutive days.
ResultsMain Outcomes Measures: sex, age, weight, height, body mass index, blood pressure and heart rate, jumping power, vertical jumping, horizontal jumping and speed 60m.
The concentric-eccentric group achieved the best results without statistically significant differences. The men improved the speed more by 60m. Women improved in jumping power, vertical jumping and horizontal jumping. Results were statistically significant if p<0.05.
ConclusionsThe group that performed the dynamic concentric-eccentric muscle work improved the performance variables analyzed further.
Women are equally improved by men and heart rate dropped to the same extent.
ClinicalTrials.gov ID: NCT03973060 (June 1; 2019)
Strength-building exercises are essential in the training and recovery of athletes.1 Strength is a physical quality that crucially influences competitive results in a wide range of sporting disciplines.2 Some studies claim that increasing muscle strength is indispensable to enhance velocity and resistance in lower-limb training programs.3–5 Several training methods have been reported with a view to optimizing the development of muscle strength.6
Explosive strength is the type of strength required in most sport disciplines and constitutes the basis for multiple technical maneuvers. In addition, it is a key factor in the performance of a significant number of athletes.7 In group sports, explosive strength is a crucial component of physical achievement as most games require athletes to make extremely fast and highly intensive movements at some point.8,9 The development of explosive strength in the knee musculature is essential for the enhancement of sprinting performance.10–12
One of the greatest breakthroughs in the area of strength-building in the last few decades has been the introduction of eccentric muscle exercises (EMT) in most training programs.13 Strength development programs are characterized by the central role played by muscle contractions but there is currently no agreement as to what type of muscle contraction is most conducive to the development of explosive strength.14
The main objective of this study analyzed different kinds of muscle training protocols divided into two main categories: dynamic muscle training, which included concentric muscle training (CMT), eccentric muscle training (EMT) and concentric-eccentric muscle training (C-EMT); and isometric muscle training (IMT). The purpose was to determine which of those protocols was most effective in enhancing explosiveness and improving athletic performance on four functional explosive strength tests: a vertical jump test, a horizontal jump test, a speed (over 60m) test and a jump force test.
Material and methodExperimental approach to the problemThis is a randomized single-blind study carried out at the Physical Therapy Department of FREMAP Majadahonda Hospital (Madrid). The recommendations of the CONSORT Declaration were adhered to in the execution of the study.15 The study variables used to respond to the objectives set were:
- •
Demographic and anthropometric variables: sex, age, weight and height.
- •
Dependent variables: systolic blood pressure (SBP), diastolic blood pressure (DBP), mean blood pressure (MBP), heart rate (HR), 60-m speed, vertical jump, horizontal jump and jump force.
- •
Independent variables: CMT, EMT, C-EMT and IMT
The size of the study sample was calculated using the EPIDAT 4.2® software. Considering that the target population was made up of 140 subjects, the sample size required for achieving a 95% bilateral confidence Interval within a 5% precision level with a 0.8 test power was established at 80 healthy and active subjects. Subjects were randomly divided into 4 sex-differentiated groups: CMT, EMT, C-EMT and IMT. Groups was made up by 20 subjects and included both men and women (Fig. 1).

Inclusion criteria: subjects had to be free from musculoskeletal lesions in the lower limb at the time of entering the study. They had to show a genuine interest in participating in the full muscle training program. They could not be enrolled in any other training plan that could interfere with the results obtained or the variables measured in this study. Exclusion criteria: hypertensive subjects or those whose blood pressure was not properly controlled at the time the study was initiated could not participate.
The study was approved by the Research Ethics Committee of the Universidad Rey Juan Carlos (Madrid), and the Science and Ethics Committee of the FREMAP Majadahonda Hospital (Madrid). Before entering the study, all the participants gave their consent by signing the relevant informed consent document, in line with the guidelines established in the Helsinki Declaration, developed by the World Medical Association (WMA) and Spanish Law 15/1999, enacted on 13 December 1999.
ProceduresAll the variables in the study were measured by a researcher who did not know which of the four study groups each subject had been assigned to.
Weight and heightA SOENHLE digital scale with a height rod, supported on a horizontal base plate, was used to perform weight and height measurements. Subjects were asked to step on the device, barefoot, in hospital pajamas and carrying nothing in their pockets. Weight was obtained in kilograms (kg) and height in centimeters (cm).
Blood pressure and heart rateAn OMRON M6 Comfort digital upper arm blood pressure monitor was used to measure blood pressure. Blood pressure was always measured at the same time. The value of the last of three consecutive measurements was recorded as the true value. This value was expressed in millimeters of mercury (mmHg).
A compact digital fingertip pulse oximeter (Shenzhen Eon Technology) was used to measure the subjects’ heart rate.
60-m speedA 60-m distance was marked on an obstacle-free sandy surface. A chronometer was used to measure this variable (in seconds [s]).
Horizontal jumpThis measurement was obtained using a smooth horizontal surface on which several lines were marked one meter apart from each other. Subjects were asked to stand on the first line with their feet hip-width apart. For a first (test) jump, subjects were required to take a leap forward with as much momentum as possible while swinging their arms and flexing their knees. After this first rehearsal, a second jump was performed whose result was recorded for the study. This result was measured in centimeters using a metal tape measure and using the first line marked on the ground and the heel of the extended foot as points of reference. The jump was not considered valid if either feet (or both) crossed the start line before taking off the ground.
Vertical jump (The Sargent Test)The protocol was as follows16: (1) First phase: subjects were asked to stand barefoot next to a straight wall and to flex their right shoulder, resting a flat hand on the wall. Subsequently, a ruler was used to measure the distance from the ground to the third finger (h1). (2) Second phase: subjects were told to cover the third finger on their right hand in blue chalk dust. They then stepped 10 centimeters away from the wall to have enough room to perform a 90° squat and move their arms about and, subsequently – and without interruption –, they performed a maximum vertical jump.17 This new distance was also recorded. This combined jump was performed three times with a 45-s break between each execution. The mean distance was calculated (h2). 3) The vertical jump value was h=h1–h2.
Jump forceThe measurement of this variable was carried out using the Sayer's validated Power Equation, which provides jump force values similar to those obtained directly when using a force Plate.18
The Sayers Power Equation is as follows:
(51.9×height CMJ (cm))+(48.9×body mass (kg))−2007
Materials required for the different kinds of muscle training:
The Tirante Musculador™ muscle belt was used for th e dynamic muscle training (EMT, CMT and C-EMT) sessions. Subjects had to stand on 40° decline platform.
The Tirante Misculador™ muscle belt allows full ext ension of the hip, which is required for active involvement of the rectus femoris muscle.19 The muscle belt provides for closed kinetic chain training, which yields the best results on vertical and horizontal jump tests; allows the subject the possibility to execute dynamic and isometric muscle movements20; and permits the performance of decline half squat exercises which reproduce a lower limb motor pattern equivalent to that of many sports maneuvers.13
The Goniometer-PRO APP for iPhone was used to verify appropriate knee positioning at the start of the test.21
Muscle training protocols used in each study group:
Prior to each muscle training session, subjects had their HR measured and were put on a 5-min stationary bicycle warm-up routine.
Subsequently, subjects in the three dynamic muscle training groups had to perform 4 series of 12 repetitions each of their assigned exercise, with 1-min rest periods between them.22 For IMT, it was agreed to follow the recommendations described by Bosco23: contraction time up to 6s; 20-s rest period between contractions; total muscle training time not longer than 12min. This type of muscle training was performed with subjects sitting on a quadriceps bench.
The training program was 12 days long. At the end of the program, all study variables were measured again.
Statistical analysisThe statistical analysis was conducted using the SPSS 21.0® for Windows software. Quantitative variables were expressed as means and standard deviation while qualitative variables were expressed as frequencies and percentages.
Gender and body mass index differences between the study groups were analyzed using the chi-squared test with Fisher's exact correction for 2×2 continuity tables (qualitative variables) and the independent samples t test (quantitative variables). Intra-group comparisons were carried out by means of an ANOVA post hoc test and the Bonferroni test.
Results were statistically significant if p<0.05.
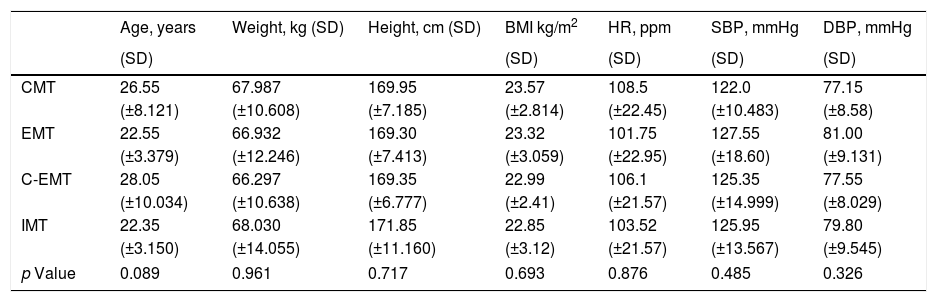
ResultsDemographic variables were homogeneous across all 4 study groups (Table 1).
Demographic data.
| Age, years | Weight, kg (SD) | Height, cm (SD) | BMI kg/m2 | HR, ppm | SBP, mmHg | DBP, mmHg | |
|---|---|---|---|---|---|---|---|
| (SD) | (SD) | (SD) | (SD) | (SD) | |||
| CMT | 26.55 | 67.987 | 169.95 | 23.57 | 108.5 | 122.0 | 77.15 |
| (±8.121) | (±10.608) | (±7.185) | (±2.814) | (±22.45) | (±10.483) | (±8.58) | |
| EMT | 22.55 | 66.932 | 169.30 | 23.32 | 101.75 | 127.55 | 81.00 |
| (±3.379) | (±12.246) | (±7.413) | (±3.059) | (±22.95) | (±18.60) | (±9.131) | |
| C-EMT | 28.05 | 66.297 | 169.35 | 22.99 | 106.1 | 125.35 | 77.55 |
| (±10.034) | (±10.638) | (±6.777) | (±2.41) | (±21.57) | (±14.999) | (±8.029) | |
| IMT | 22.35 | 68.030 | 171.85 | 22.85 | 103.52 | 125.95 | 79.80 |
| (±3.150) | (±14.055) | (±11.160) | (±3.12) | (±21.57) | (±13.567) | (±9.545) | |
| p Value | 0.089 | 0.961 | 0.717 | 0.693 | 0.876 | 0.485 | 0.326 |
CMT: concentric muscle training.
EMT: eccentric muscle training.
C-EMT: concentric-eccentric muscle training.
IMT: isometric muscle training.
BMI: body mass index.
HR: heart rate.
SBP: systolic blood pressure.
DBP: diastolic blood pressure.
Both systolic (SBP) and diastolic (DBP) blood pressure was measured for all the subjects in the study.
The relative decrease of SBP and DBP following the 12-day training program was analyzed in the subjects assigned to the dynamic muscle training groups.
HR was measured before and after each exercise during the 12-day training program.
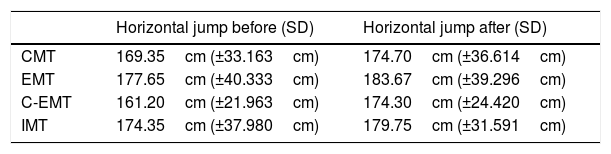
The functional explosive strength tests were administered before and after the 12-day training program (Table 2).
Values of the 4 tests analyzed before and after muscle training.
| Horizontal jump before (SD) | Horizontal jump after (SD) | |
|---|---|---|
| CMT | 169.35cm (±33.163cm) | 174.70cm (±36.614cm) |
| EMT | 177.65cm (±40.333cm) | 183.67cm (±39.296cm) |
| C-EMT | 161.20cm (±21.963cm) | 174.30cm (±24.420cm) |
| IMT | 174.35cm (±37.980cm) | 179.75cm (±31.591cm) |
| Vertical jump before (SD) | Vertical jump after (SD) | |
|---|---|---|
| CMT | 40.01cm (±11.18cm) | 42.74cm (±10.934cm) |
| EMT | 40.40cm (±9.598cm) | 40.65cm (±9.706cm) |
| C-EMT | 36.90cm (±9.504cm) | 40.21cm (±7.766cm) |
| IMT | 42.74cm (±11.71cm) | 43.96cm (±10.941cm) |
| Jump force before (SD) | Jump force after (SD) | |
|---|---|---|
| CMT | 3,393,785 (±936,357) | 3,535,592 (±919,223) |
| EMT | 3,362,906 (±978,498) | 3,366,804 (±1,010,068) |
| C-EMT | 3,148,710 (±758,534) | 3,453,398 (±742,506) |
| IMT | 3,538,225 (±1,188,107) | 3,593,745 (±1,115,361) |
| Speed before (SD) | Speed after (SD) | |
|---|---|---|
| CMT | 9.25s (±1.623s) | 8.85s (±1.419s) |
| EMT | 9.06s (±1.369s) | 8.66s (±1.101s) |
| C-EMT | 9.15s (±1.090s) | 8.74s (±7.766s) |
| IMT | 8.81s (±1.369s) | 8.58s (±1.391s) |
CMT: concentric muscle training.
EMT: eccentric muscle training.
C-EMT: concentric-eccentric muscle training.
IMT: isometric muscle training.
The relative improvement achieved by men was compared to that achieved by women for different variables analyzed showing in horizontal jump before training in men values of 194.5cm respect 146.77cm in women, being after training for men 201.46cm and 154.75cm for women. In vertical jump, the data before training were for men 47.29cm and 32.73cm, for women, corresponding after training to men 49.24cm and 34.55cm in women. Speed also showed improvement, in men before training 8.03s being 7.74s after training. In women, the speed was 10.11s before and 9.68 after training. Finally, in jump force, before training the data of men were 4155.07 and 4253.1 in women, and after 4253.1 in men and 2662.34 in women (Table 3).
Mean values for the different variables analyzed for each gender.
| Horizontal jump | Before (SD) | After (SD) |
|---|---|---|
| Men | 194.50cm (±25.83cm) | 201.46cm (±24.33cm) |
| Women | 146.77cm (±22.57cm) | 154.75cm (±22.40cm) |
| Vertical jump | Before (SD) | After (SD) |
|---|---|---|
| Men | 47.29cm (±8.31cm) | 49.24cm (±7.37cm) |
| Women | 32.73cm (±6.90cm) | 34.55cm (±5.62cm) |
| Speed | Before (SD) | After (SD) |
|---|---|---|
| Men | 8.03s (±0.683s) | 7.74s (±0.648s) |
| Women | 10.11s (±1.03s) | 9.68s (±0.913s) |
| Jump force | Before (SD) | After (SD) |
|---|---|---|
| Men | 4155.07 (±630.39) | 4253.10 (±588.55) |
| Women | 2566.74 (±458.52) | 2662.34 (±419.06) |
At the end of the training program, comparisons were made to determine the differences between the groups. Specifically, comparisons focused on the improvements achieved by individual subjects and by the study groups on completion of the exercise sessions.
On the horizontal jump test, the comparison between the scores achieved before and after the training program proved statistically significant (p<0.001).
For the vertical jump test, statistically significant results were obtained when comparing the pre- and post-training scores of individual subjects but not when comparing the study groups themselves (p<0.001).
On the 60-m speed test, individual comparisons between pre- and post-training scores showed statistically significant differences but comparisons between the groups did not. Likewise, no statistically significant differences were observed when comparing the improvement achieved on vertical jumping with the improvement achieved on the 60-m speed test (p<0.001).
For the jumping variables, it was intended to know the relationship between having lost weight during the 12 days of muscle training and jumping more on the last day of assessment. The results obtained do not show statistically significant differences between the subjects who lost weight versus those who gained weight, both in the horizontal jump (p=0.920), nor in the vertical jump (p=0.775).
On the jump force test, individual differences between pre- and post-training scores were statistically significant, whereas the differences between the groups were not. The subjects’ HR was measured every day. Pre- and post-training HR values were compared daily for each subject. In addition, comparisons between day 1 and day 6 (pre- and mid-program) HR values and between day 1 and day 12 (pre- and post-program) HR values were drawn. The results obtained were: between day 1–6, the HR before training p=0.269 and after p=0.174; between day 1–12, HR before training p=0.237 and after p=0.063.
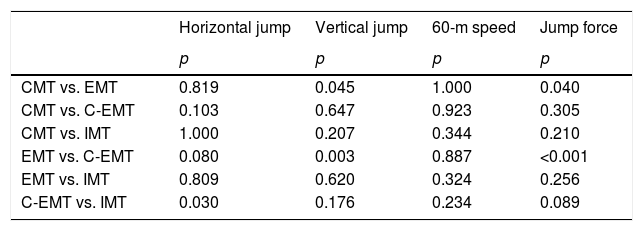
Variables analyzed for each study groupAn analysis was conducted of the differences between study groups with respect to the variables considered to determine which of the groups obtained the most effective results from the training they engaged in Table 4.
Comparison of the increases achieved by all study groups with respect to the variables analyzed.
| Horizontal jump | Vertical jump | 60-m speed | Jump force | |
|---|---|---|---|---|
| p | p | p | p | |
| CMT vs. EMT | 0.819 | 0.045 | 1.000 | 0.040 |
| CMT vs. C-EMT | 0.103 | 0.647 | 0.923 | 0.305 |
| CMT vs. IMT | 1.000 | 0.207 | 0.344 | 0.210 |
| EMT vs. C-EMT | 0.080 | 0.003 | 0.887 | <0.001 |
| EMT vs. IMT | 0.809 | 0.620 | 0.324 | 0.256 |
| C-EMT vs. IMT | 0.030 | 0.176 | 0.234 | 0.089 |
CMT: concentric muscle training.
EMT: eccentric muscle training.
C-EMT: concentric-eccentric muscle training.
IMT: isometric muscle training.
An analysis was made of the differences displayed by each of the dynamic muscle training groups with respect to the four variables studied to identify the group where the training routines were most effective. Statistically significant values were obtained in the comparison of CMT vs. EMT for the vertical jump with a p=0.045 and for the jump power with a p=0.040, and in the comparison of EMT vs. C-EMT for the vertical jump and power jump with a significance of p=0.003 and p<0.001, respectively.
Gender-based analysis of the variablesA determination was made of which of the two genders (men vs. women) achieved the greatest improvements on each of the functional tests administered: horizontal jump (p=0.782), vertical jump (p=0.297), speed (p=0.009) and jump power (p=0.326).
Blood pressure and heart rate- •
A comparison was made between the dynamic muscle training groups and the IMT group to determine any differences on the following parameters:
- •
SBP and DBP: at the end of the study, we checked if both systolic and diastolic pressure, were significantly different between both working methods (dynamic vs. static), showing for SBP p=0.631 and DBP p=0.941.
- •
MBP: the differences between the dynamic muscle training groups and the IMT group were not statistically significant with respect to this physiological parameter (p=0.831).
- •
HR: HR values were measured all along the 12-day program both in the groups where subjects did their training while standing (dynamic groups) and in those where they were seated as they did their exercises (isometric group). The differences between the values recorded were statistically significant: HR1 p=0.007, HR6 p=0.003 and HR12 p=0.002.
The vertical jump, the horizontal jump, the 60-m sprint and jump force were selected as variables for this study on account of the direct relationship that exists between them. In 2004, Wisloff demonstrated a close relationship between the vertical and the horizontal jump.24 In the present study, that kind of direct relationship between variables was not observed, which means that an improvement on one variable does not necessarily entail an improvement on the others.
An analysis of the values obtained before and after the study for each of the variables considered shows that it was the C-EMT group that experienced the greatest improvement, although differences with the other groups were not statistically significant. It must be borne in mind that both the pre-training and post-training values recorded in all four groups for the different variables were very similar. In addition, differences between pre- and post-training values were scarce. In line with other authors, the present study came to the conclusion that combined muscular training (C-EMT) is the most effective type of training for improving explosive strength performance. Dudley et al. claim that training sessions that combine concentric and eccentric exercises are cumulatively more effective than training consisting solely of isolated concentric and eccentric actions.25
For their part, Friedmann et al. compared two groups of athletes for 6 weeks and found that the group who combined concentric and eccentric exercises obtained the best results on vertical jump tests, suggesting that combined training results in an enhanced development of explosive strength.26 The present study did not find a statistically significant relationship between weight loss and greater explosive strength improvements on the vertical jump, which differs from the findings by Viitasalo et al.27
Notable differences were found in the vertical jump scores between males and females. Most of the evidence indicates that the mean absolute upper and lower trunk strength scores obtained by women are lower than those observed in men. Nonetheless, this difference takes on different forms as a function of the type of muscle movement performed. In this respect, the results obtained by males and females following eccentric exercises exhibit more similarities than those observed following concentric exercises.4,28
In the present study, males achieved a relative explosive strength gain of 3.45% on horizontal jump tests, whereas the improvement achieved by women was 5.5%. Fort the vertical jump, the relative gain obtained by men was 3.96%, while women obtained an improvement of 5.27%. On the 60-m speed test, the relative improvement attributed to males was 3.61%, while women increased their baseline values by 4.25%. For jump force, men recorded a 2.30% improvement while women reached 3.59%. In line with our findings, previous studies show that dynamic muscle training is equally beneficial for both genders, with a slight advantage in favor of women.29,30
However, this advantage in favor of women seems to disappear with isometric muscle training. In fact, in these exercises’ men, probably on account of their greater muscle mass, usually obtain higher scores than women. In this study, men obtained significantly better scores than women on the vertical jump test. This could be since women have 10% more adipose tissue than men in the lower limbs, which means that muscles in that area are more strained as a result of the extra load they have to bear. It has not been possible to confirm this hypothesis as the only report in the literature that has found a similar advantage of men over women did so for upper extremities.29 In any event, the most striking differences between males and females were observed in the dynamic muscle training groups and not in the IMT group and could be attributed to the effect of testosterone, which stimulates the nervous system and favors the phenotyping of rapid fibers.31
The heart rate and blood pressure values observed were remarkable. Following dynamic muscle training, a series of adaptative changes were recorded, which consisted in a reduction in HP both at rest and after exercise32 and a decrease in BP.33 A reduction was observed in the mean HR values of all groups from the day before the start of training until the day after cessation.
Nevertheless, the finding that resting HR decreases as the training session progresses, reported in this article and in the above-mentioned studies, only seems to hold when muscle training is performed in short sessions at low-to-moderate intensity.34 Conversely, the effects of long-term muscle training are unclear, with some studies even reporting no observable changes in the subjects’ HR.35,36
MBP values also decreased in all study groups, with the most notable differences corresponding to SBP in the C-EMT group.
Isometric activity has traditionally been associated with extreme responses in hypertensive individuals. Brook et al.,37 showed that this type of muscle training could become a useful non-pharmacological tool in the treatment of subjects with high BP. These authors reported a decrease of nearly 6mmHg following isometric training, supporting the recent inclusion by the American Heart Association of isometric exercise as BP-lowering treatment. Even if there were no hypertensive subjects in the patient sample used for this study, both SBP and DBP values in the IMT group also diminished.
At the level of dynamic muscle exercises, there is significant evidence to suggest that a certain reduction of resting SBP and DBP occurs following a bout of muscle training.38,39 This reduction ranges between 2 and 4mmHg for SBP and DBP respectively, which entails a 2% reduction of SBP and a 4% reduction of DBP.39
All three dynamic muscle training groups in this study also experienced a reduction of resting MBP. As to the percentage of BP reduction, results were similar to those reported by Bailon et al.40
All study groups exhibited a decrease in both HR and BP values. As dynamic muscle training was performed standing up and the static training was carried out sitting down, it could be inferred that the reduction in HP and BP values would exhibit differences depending on which group subjects were in. For SBP, DBP and MBP no statistically significant differences were observed between performing the muscle-building exercises in a standing or a sitting position. However, when the HR parameter was analyzed, statistically significant differences were found between dynamic and static muscle exercises in favor of the latter. The most significant decrease in HR occurred in the group that trained in a seated position. Some authors have explained this finding by arguing that activities performed sitting down or lying are associated with a decrease in hydrostatic pressure, which facilitates venous return to the heart and requires less effort thereby reducing the HR.27
ConclusionsConcentric-eccentric dynamic muscle training produced the best results on the analyzed variables. On the 60-m speed variable, the results of all three dynamic muscle training groups were better than those obtained by the isometric group, albeit the difference was not significant.
Gender-wise, it was the women who obtained the greatest improvement on their initial scores. This said, the men showed a better vertical jump performance than women, with the latter obtaining better results on horizontal jump tests and ran the 60m distance faster than men.
During the sessions, the HR experimented a progressive short-term reduction, which was particularly striking in the dynamic muscle training groups. As regards blood pressure, MBP values diminished across all study groups.
Conflict of interestThe authors declare that they don’t have any conflict of interests.
Hospital where the research was conducted: FREMAP-Majadahonda Hospital Carretera de Pozuelo, 61, 28222 Majadahonda (Madrid, Spain).

