







El presente estudio tiene como objetivo describir las características del programa «Menorca borina’t» («Menorca muévete») diseñado para promocionar la actividad física y el ejercicio físico a fin de mejorar la salud de la población. El programa liderado desde el Gabinete de Medicina Deportiva del Consell Insular de Menorca, se estructura en 4 niveles de actuación que abarcan las siguientes áreas: educativa (intervenciones dirigidas a las escuelas y aulas de educación primaria); comunitaria (acciones que abarcan diferentes sectores de la sociedad, destacando la creación de una red de rutas urbanas saludables e intervenciones relacionadas con la movilidad sostenible); prescripción de ejercicio físico (colaboración con atención primaria para prescribir ejercicio físico en sujetos con factores de riesgo cardiovascular), y científico-académica (labor de formación continuada para profesionales sanitarios). El fomento y la dinamización de estas estrategias interdependientes es de esperar que redunden en un beneficio a escala global en la salud de la población.
The objective of the present study is to describe the characteristics of the “Minorca borina’t” (“Minorca move yourself”) program, which was designed to promote physical activity and exercise to improve the population's health. The program led by the Department of Sports Medicine of Minorca Insular Council was divided into four levels of performance, which include the following areas: educational (interventions directed at schools and primary education classrooms); community (actions encompassing different sectors of society, including the development of urban healthy walking routes and interventions related to sustained mobility); prescription of physical exercise (cooperation with Primary Care Centres for prescribing physical exercise to subjects with cardiovascular risk factors); and scientific-academic (continuing education activities for healthcare personnel). Intensifying and promoting these interdependent strategies is expected to result in global benefits to population health.
A sedentary lifestyle and the lack of regular physical exercise are widely recognised to be a pressing health problem worldwide. This is not solely due to its involvement as a risk factor in cardiovascular morbimortality, but also because it adds to the healthcare and economic burden involved in managing the main chronic non-infectious diseases. The devastating effects of the worldwide sedentary lifestyle pandemic have given rise to an increasing demand for effective strategies to increase the levels of physical activity and exercise in the population.
The World Health Organisation (WHO) has estimated that physical inactivity causes a total of 1.9 million deaths worldwide, and that 47% of global mortality can be attributed to only 20 risk factors. Of these, a sedentary lifestyle stands in seventh place.1 The European Union Eurobarometer 412 survey2 was carried out in 2013 with the participation of 27,919 citizens of the 28 member countries. It found that 59% of citizens never or rarely practice sport or some type of physical activity, while 13% do not even walk at least 10 min per day and 69% remain seated during from 2.5 to 8.5 h a day. On the other hand, physical activity falls markedly with age, so that in the age group over 55 years old 70% of the men and 71% of the women never or rarely do sport. Lack of time was the reason for inactivity given the most often (42%), followed by lack of interest (20%) or suffering a disease (13%). The results of this survey were very similar to those obtained in a previous survey in 2009.
As a consequence of these alarming reports, which urge the need for measures that promote and facilitate physical exercise, a wide range of local, regional and national government bodies, the majority of which are in first world countries, have developed plans and models to stimulate and promote physical activity among their populations.3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16 In Spain the Consejo Superior de Deportes created the A + D Plan to guarantee that the entire Spanish population has universal access to high quality sports facilities, to combat the widespread sedentary lifestyle and obesity, as well as to promote active healthy lifestyle habits.17 This plan covers the period from 2010 to 2020 and intends to reach all citizens through actions that involve and affect everyone in general as well as specific programs for certain groups. Likewise, regulatory, planning and executive powers are held by the corresponding sectors in the Autonomous Communities. The National Plan for Promoting Physical Activity (PNPAF) in Catalonia,17, 18, 19 the Basque Plan for Physical Activity in Euskadi20 or the ACTIVA Community Program for the prescription of physical exercise in the Region of Murcia21 are examples of the development and implementation of these initiatives.
Data on the physical activity of the population in the Balearic Islands were gathered in the ISIB07 survey that was promoted by the regional government.22 This survey was conducted face-to-face in interviewees’ homes, in a population stratified according to census units and representative sizes of population of the four islands, with a total of 2233 interviews. The following results stand out in connection with physical activity: 54.4% of the population do not do a desirable amount of physical exercise, and the reason for this given the most frequently is lack of time. 24.8% of the population over the age of 15 years old stated that they are seated during their main activity, and 41.7% spend most of the day standing without walking long distances. Young people and those over the age of 65 years old are the one who spend the majority of the day sitting. Respecting physical activity in their free time, 57.2% of the population stated that they do perform some type of physical activity in their free time, although this percentage falls with age. In the segment of the population aged from 5 to 15 years old, 11.3% do no physical activities in their free time and 89.7% watch television every day (three quarters of them for 1 h or longer). The response to this evidence was to develop and implement a sport policy model as a priority line of action of the Sports Medicine Office of the Sports Department of the Consell Insular, Minorca. This work therefore aims to describe the general characteristics of a program to promote physical activity for health, in a highly particular context like the Island of Minorca. It also contains a general description of each area affected by the implementation of the said model. The name, “Menorca borina’t (move yourself)”, was chosen as a clear and expressive means of getting attention and communicating the purpose of the program (Figure 1)

Figure 1. Program logotype.
Geographical and demographic situation, together with healthcare resources on the Island of MinorcaMinorca is the most Eastern and Northern of the Balearic Islands (Spain). It measures 700 km2, with a perimeter of less than 200 km and a total population of 91,601 inhabitants.23 For administrative purposes it is divided into 8 townships, while geographically it consists of small population centres. Three public administrations govern policies on the island: the Consell Insular de Menorca and the town halls control the area of sports, while the Balearic Islands Government controls healthcare. These different areas of government affect how resources are managed, together with physical exercise programs and physical activities. The health facilities on the island consist of nine Health Centres-Basic Health Units and a General Hospital General managed by the Govern Balear Board of Health. The only Sports Medicine Centre belongs to the Sports Department of Menorca Consell Insular. It has a doctor specialising in Sports Medicine and a graduate in Physical Activity and Sports Science.
Foundations for the implementation of the “Menorca borina’t (move yourself)” program and its objectivesAlthough there is a clear relationship between habitual physical activity and health, this is based on lifestyle characteristics in which subjects’ environment is especially important. There are many factors that prevent subjects from being more physically active, and some of them increasingly hinder the creation of healthy active habits in the population. Political strategies to reduce the morbimortality of non-infectious chronic diseases have to include the importance of lifestyle and how to influence this. The necessary resources have to be assigned proportionately within the framework of the different health system organisations.24 Causal factors must also be studied, together with those associated with physical inactivity, so that specific actions aimed at these targets can be designed. The recently recommended ecological models take a broader view of lifestyle causes.25 They therefore include the social and physical environment as contributors to physical inactivity, most especially those outside the health sector. These include town planning, transport systems and parks and paths. On the other hand, the need for policies designed to promote actions that gradually increase physical activity has been emphasised, starting with interventions that are monitored to prove their efficacy and which become rooted in society.3
Given the above background and following consultation of the strategies of other programs to encourage physical activity in our area, especially the Catalonia PNPAF,17, 18 as well as the “Agita São Paulo” model based on interventions at different levels to encourage physical activity among the 37 million inhabitants of São Paulo State, Brazil,5 we designed the “Menorca borina’t (move yourself)” program.
Based on the knowledge that the possibilities of influencing an individual depend on multiple factors, this program to promote physical activity for health uses a multicomponent and multisectorial model. In this model actions and different types of intervention function synergically and are more effective than the implementation of isolated measures.26
The aims of this program are: (a) to improve levels of physical activity and quality of life in the population of the Island of Minorca; (b) to ensure that the participants in the program have an active and healthy lifestyle; (c) to create a collaborative link between the different administrative bodies involved in health and sport in the island of Minorca; and (d) to ensure that the program reaches the largest possible number of inhabitants.
As was pointed out in Figure 2, this model acts on four areas of intervention: Education, Community, the Prescription of Physical Exercise and Scientific-Academic questions.
Figure 2. Program structure.
The area of educationPhysical inactivity and a poor diet begin during childhood and youth, leading to high rates of being overweight and obesity in the population under the age of 15 years old.27 On the other hand, in infancy and adolescence subjects are more open to learning and are able to incorporate lifestyle habits that may consolidate over time (physical activity and diet, etc.), Kelder et al. (1994) find that habits become quite firmly fixed before the age of 11 years old.28, 29 Education for health has been widely recommended as the most effective way to promote the adoption of healthy lifestyles over the long term.30 In this way, the promotion of health in schools is one of the key tools in health interventions. In a universal education system the inclusion of obligatory curriculum contents that promote and educate about health therefore allows this action to reach the population aged from 4 to 14 years old, independently of other factors such as sex, class or parental educational level. Teachers are able to act as health-promoting agents, and they are highly qualified to play this role. The Organic Law to improve the quality of education (LOMCE 2013) includes this aspect among the skills that students have to acquire.31
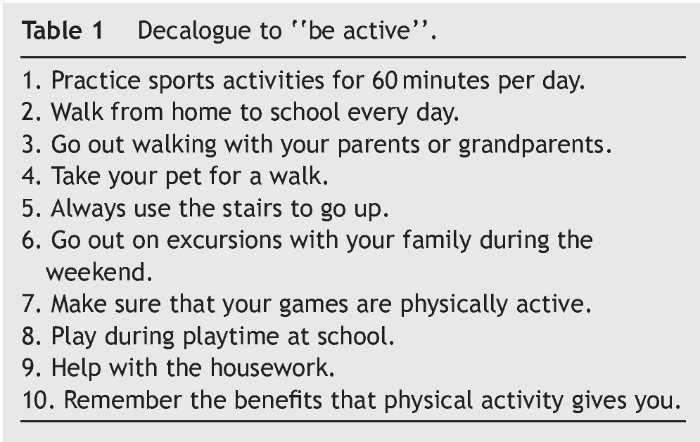
Given the above considerations, the educational actions included in the “Menorca borina’t (move yourself)” program consist of designing theoretical-practical workshops to be given by Menorca Consell Insular within the framework of the Young Health and Culture program (Salut Jove i Cultura). This is aimed initially at pupils in their 3rd and 4th years of primary school (8–10 years old) before being extended to cover other ages and educational stages. These workshops take place in schools during the school timetable and include a theoretical explanation lasting for 60 min and the presentation of a list of good practices to be active (Table 1). They also include a practical part with a walk along healthy urban routes. Broadly speaking, these workshops include an explanation of the health problems which arise due to a sedentary lifestyle and a description of the benefits of an active lifestyle and plasticising physical exercise, presenting different way of promoting physical activity for health with the aim of getting those taking part to follow this proposal. Thus the students themselves become physical activity promoters within their school and immediate family environment.
Physical activity as a strategy for promoting health is a complete social and political process.32 At community level the emphasis is on seeking effective strategies that are able to increase the level of physical activity in the population. Increasing interventions are therefore necessary in broad areas of public policy such as town planning, education, culture, free time, the environment, transport and, of course, health, to move society towards a more active lifestyle.
Activities in the community include the creation of healthy routes and different actions in the media and social bodies to publicise and spread awareness of the “Menorca borina’t (move yourself)” program.
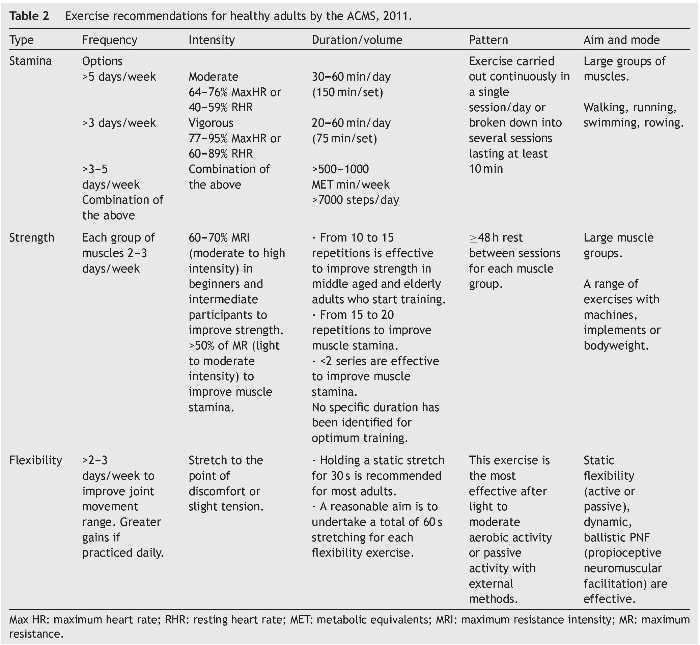
The healthy routes consist of the creation of a network of 17 measured and properly signposted urban routes, to offer the population healthy paths they can use freely as sports facilities. Quantifiable physical exercise is possible on these routes, thereby motivating people who are not very active to walk along them and achieve the health recommendations for young people and adults, following the American College of Sports Medicine, ACSM guides33 (Table 2). A total of 60 km of healthy urban routes are available in the municipalities of the island, thereby forming a “micro-globalisation” of the whole Minorcan territory. The design took into account the recommendations for urban routes of this type, such as running within towns, the distances to be covered, a suitable accumulated change of altitude, accessible paths and the presence of trees and benches for resting, as well as the fact that they should start at the health centre and/or sports pavilion of each town.34 All of these routes fulfil certain technical criteria that make them safe and suitable for anyone, with a minimum length corresponding to approximately 30 min, good illumination, wide paths with a minimum of interruptions for walkers and without any architectural barriers.
To facilitate access to these routes, a special tile is set into paths that shows the program logotype (Figure 3). This tile differs in colour depending on the length of the route, while a vertical display on the front of the health centre and/or sports pavilion shows a map of the routes in the town, their technical characteristics and information of interest. The tile also shows the web address www.rutessaludables.com so that it is possible to access the map of the island and select the town to walk in. This internet portal can also be used to obtain information on routes, downloading them in pdf format or creating a virtual route.
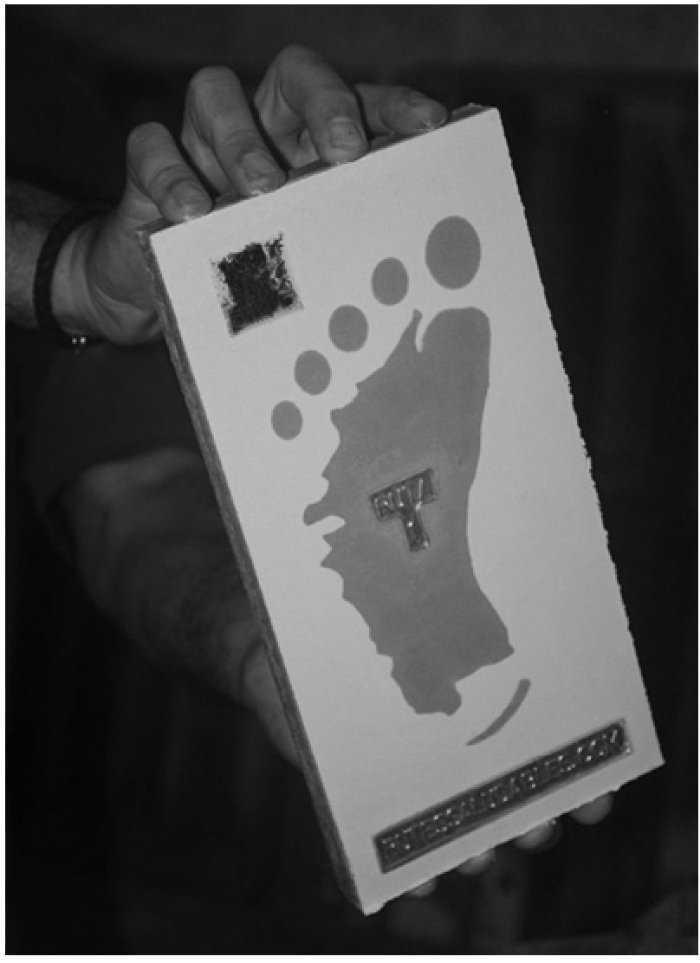
Figure 3. Program tile used to mark healthy routes in the island towns.
The opening of the healthy routes in each town was publicised in the media (local newspapers, press conferences and local TV, etc.), as well as the distribution of leaflets by the Town Sports Department, primary care health staff and doctors in the general hospital of the island. This was completed by the publication of physical activity for health promotional materials in the local press and magazines, together with the diffusion of physical exercise and healthy lifestyle promotions in the media, keeping the website and social networks of the Sports Department of Menorca Consell Insular.
Other community activities include actions to promote a healthy lifestyle and the practice of physical exercise in citizens’ associations and social bodies. These centre chiefly on conferences, going for group walks and practical workshops. Respecting healthy companies and in the field of work in local government bodies, Menorca Consell Insular and the town halls have designed workshops to be held during working hours, preparing posters for display at decisive points and creating “healthy messages”. The latter contain brief information about how acquiring active habits to improve health, and they are published by the Human Resources Department of Menorca Consell Insular. Other interventions include multi-population events such as celebrating “world physical activity day” or the “sports fair”, which have the aim of raising the awareness of the population about the importance for fitness of achieving a healthy level of physical activity. A series of physical activities are organised involving different sports, with the help of local public administrations. These include group walks, races, gym sessions, zumba, gerontogym or free use of municipal sports facilities, inviting everyone to take part.
Prescribing physical exercisePrescribing physical exercise (PPE) is one of the pillars of our program. Its main aim is to ensure that participants follow an active lifestyle. This type of PPE is aimed at individuals who are adult, sedentary, with no known disease and one or more cardiovascular risk factors, a suitable level of motivation (stages 3: preparation, and 4: action, of the transtheoretical model health behaviour model of Prochaska and Diclemente35) and who are prepared to take part in a controlled program of physical exercise36 to increase their daily physical activity. The program lasts for 9 months and the progress of participants is checked at 3, 6 and 9 months, to monitor their physical fitness and health parameters.
The subjects were recruited in the Primary Care Centre by family doctors and nurses, who referred them to Menorca Consell Insular Sports Medicine Office. Subjects there were fully evaluated by the specialist Doctor in Sports Medicine and the graduate in Physical Activity and Sports Science, so that they could be prescribed the most suitable physical exercise routine. The characteristics of the initial evaluation, physical exercise planning and control and monitoring of the participants are described below.
The initial medical-sports health evaluationThe type of physical exercise to be prescribed is based on previous evaluation of the subject's cardiovascular risk. According to the recommendations of the ACSM37 this is classified as low, moderate or high, depending on their age and the number of risk factors present. Their quality of life was also self-assessed in the physical and mental sections of questionnaire SF-12.38 The medical-sports examination includes a clinical history with anamnesis, physical examination, anthropometrics (weight, height, body mass index, abdominal perimeter and skin folds), cardiorespiratory examination (cardiac and pulmonary auscultation, blood pressure, functional examination with forced spirometry and 12 derivation resting electrocardiogram [ECG]) together with analysis of biochemical health markers and lipid profile. Depending on the results of the resting ECG, and if the degree of cardiovascular risk is moderate or high, an effort test was applied with 12 deviation monitoring using a cycle ergometer to evaluate cardiovascular adaptation to physical effort.
Initial evaluation of physical fitness and conditionThe International Physical Activity Questionnaire (IPAQ) was used to determine how much physical activity adults usually do.39 This instrument makes it possible to estimate energy expenditure during a working day and free time, establishing a classification of physical fitness that runs from sedentary to very active.
Five AFISAL-INEFC battery tests for healthy adults are used to evaluate physical condition.40, 41 These include standing on one leg without vision, flexibility, maximum grasping strength (manual dynamometer), lower limb strength and aerobic stamina (test of walking for 6 min). Older individuals and those with a greater degree of physical inactivity do the test of standing on one leg with vision.
The prescription of physical exerciseOnce the initial evaluations have been performed the sports medicine specialist prescribes an exercise program with certain characteristics and intensity, after which the Physical Education graduate designs the physical exercise plan corresponding to each individual. Taking into account the fact that the participants are sedentary or not very active and at a low level of physical fitness, the basic program is designed for light to moderate physical exercise at from 3 to 5.9 METs (metabolic equivalents), (60–75% of maximum heart rate) and vigorous physical exercise of ≥6 METs (75–85% of maximum heart rate). The aim is to increase energy expenditure up to 1500–2000 kcal/week or 500–1000 METs/week (Table 2). The physical exercise program includes cardio-respiratory stamina, flexibility and strength.
The cardio-respiratory stamina exercise consists of walking for 30–60 min per day, in a single session or accumulating sessions at least 10 min long, up to 90–420 min/week during 3–7 days/week, depending on the availability of participants, or to attain 10,000 steps per day. In the first 12 weeks participants walk at a constant speed to achieve the necessary cardiorespiratory and muscular adaptation, after which interval training starts on 2–3 days per week. Each interval training session lasts for 10–20 min, with a total of 75 min/week of vigorous exercise, alternating with aerobic work at a constant speed. There is a 5–15% weekly increase in volume until 12–24 weeks.
Flexibility is worked on by different static stretching exercises lasting 20–30 s, in 1–2 series of five exercises of large muscle groups after walks or toning routines. Given the lack of experience and strength of the participants, together with the probability that they would have to do the exercise alone, they were given few exercises to do, to ensure correct technical execution and safety. The exercises involve different planes of movement, combining pulling and pushing using elastic bands and free weight.42 With 10–20 repetitions in from 1–4 series, 2–3 days per week and resting at least 48 h between sessions for each group of muscles.
The following elements are used to control the intensity of training: (1) circuits for walking (healthy routes); (2) pulsometers and accelerometers to control the intensity of walking and the number of steps per day, respectively. Pulsometers and accelerometers also play a useful role in motivation; (3) Borg's perceived effort scale43; and (4) a personal record sheet so that users can keep a daily record of the prescribed parameters. This also functions as a feedback mechanism.
Monitoring the physical exercise programIn the first check the participant is given the necessary material for the first month of their physical exercise program, and they have to record the exercise actually done. Monthly checks are established until the sixth month, when the anthropometric variables are measured again, together with a follow-up analysis. From the sixth month to the ninth month checks are performed by telephone or face-to-face, decided by the doctor. The last visit at 9 months includes a medical examination and final analysis, together with repetition of the physical tests and the IPAQ and SF-12 questionnaires. The final report shows the progress made, and the participant is given a copy of this report for their family doctor. In this last visit the participant is encouraged to continue with physical exercise, or they are advised about selecting another sports activity.
To maintain motivation for the habitual practice of physical exercise during and after taking part in the program, a contact group has been created with all of the participants. A mobile telephone messaging application keeps them informed about healthy physical activities that are organised, as well as news in connection with physical activity and health, and “reminder” messages for them to stay active. On the other hand, this group can also be used to contact other participants and create independent groups of walkers.
The scientific and academic areaThis area includes all of the activities involved in publicising knowledge in connection with the habits of a healthy lifestyle, physical exercise and its association with improving the health of the population. More specifically, a Day on Physical Activity and Heath is held every year within the context of Minorca Public Health School. The activities of Minorca Public Health School take place in Lazareto de Maó, and they are organised jointly by the Menorca Consell Insular, the Govern Balear, the Universitat de les Illes Balears and the Ministry of Health, Social Services and Equality, through Carlos III Health Institute. This day offers room for debate about current strategies and the creation of new proposals for actions in promoting physical activity for the health of the population. Health science professionals take part in these talks, together with those who work in the field of physical exercise and sport and technical personnel in the areas of health and sport in local and regional government bodies.
ConclusionsThe public administration faces the challenge of guiding work in active preventative policies aimed at promoting physical activity and physical exercise to improve health.
The “Menorca borina’t (move yourself)” project commenced with the design and marking of healthy urban routes in the towns of Minorca, using a basic element in the environment closest to citizens such as urban architecture to promote physical activity. It has to be accepted now that health promotion cannot be exclusively the task of healthcare professionals, as it is shared with other parts of the community. It is therefore necessary to seek links and alliances between all social sectors to ensure that the message reaches citizens and that they themselves are able to take decisions about their lifestyle. A very wide range of social sectors have to be involved to add to the value of physical activity as a means of improving health. They include town planning, public transport, local businesses and media, among others, to raise the awareness of the population in the fight against a sedentary lifestyle.
The “Menorca borina’t (move yourself)” program is a call to the island's inhabitants to be more active physically. It uses the Minorcan word “borina’t” to encourage people to do something more for their health and not to be either physically or mentally static, adopting a more active everyday lifestyle and abandoning more sedentary attitudes which are bad for the health, as well as including and following healthy eating practices that are typical of our traditional Mediterranean diet. Although the results and evaluation of the program are not yet available, this proposed lifestyle and the environmental ecology of Minorca may consist of the creation of a particular and different “active lifestyle ecosystem”.8
Conflicts of interestThe authors declare that they have no conflict of interest.
Acknowledgement
We would like to thank Dr. Marta Pulido for her help in writing and revising the manuscript.
Received 11 May 2017;
accepted 26 July 2017
Available online 11 November 2017
∗ Corresponding author.
E-mail address: gabinet-medesport@cime.es (F.S. Portella).

