






El objetivo de esta revisión es analizar la influencia de la sensibilidad plantar en la mejora de la capacidad de reequilibrio y de gestión del movimiento, analizando los mecanismos que permiten valorarla y describiendo los factores que en ella influyen. Para ello se realizó una búsqueda sistemática de la bibliografía publicada entre 2000 y 2016, en las bases de datos PubMed, Web of Science, SPORTDiscus y en las referencias citadas en los artículos recuperados, cuyo idioma de publicación fuera español o inglés. Un total de 9 artículos fueron recuperados y analizados.
La mayoría de los estudios sugieren que la retroalimentación sensorial del pie resulta fundamental en el mantenimiento de los patrones generales (posturales y de desplazamiento) y específicos (deportivos). La alteración de la cantidad o calidad de la información aferente plantar no solo parece alterar la creación de los diferentes patrones, sino que podrá incrementar el riesgo de aparición de lesiones.
The objective of this review is to analyse the influence of plantar sensitivity in improving the ability to re-balance and manage movement by analysing the mechanisms available to assess this and describing the factors that influence this. This project required a systematic search of the literature published between 2000 and 2016 in PubMed, Web of Science, and SPORTDiscus, as well as the references cited in relevant articles from these sources. The publication languages were Spanish and English, and a total of 9 items were collected and analysed.
Most studies suggest that sensory feedback from the foot is essential in maintaining general (postural and displacement) and specific (sport) patterns. Altering the quantity or quality of plantar afferent information not only appears to alter the creation of different patterns but may also increase the risk of injury.
Introduction
The foot is a hypercomplex structure which supports the body and is characterised by being the only body part in contact with the ground. Among its various functions a key one is to provide afferent information to the central nervous system from plantar receptors, which will then be used to maintain posture and produce movement patterns. In recent years, several lines of research have focussed on the study of the influence that afferent information from the plantar receptors of the somatosensory system exerts on balance, postural control and movement, as well as on the occurrence of lesions.1-4 Taking into account that the sole of the foot forms the point of contact between our body and the surface which supports it, and that it also has a large number of sensitive receptors, it is logical to assume that the sole of the foot will be directly involved in the management of posture and movement.5,6
The skin is the largest organ in the human body.7 Its function is to act as a protective barrier, isolating the body from the surrounding environment, protecting it and contributing to maintaining its structures intact, while acting as a highly efficient communication system between the body and the immediate environment. In addition, the skin of the foot has certain characteristics that differentiate it from that of the rest of the human body: firstly, its epidermis presents greater thickness, which contributes to improving its resistance and its ability to cushion the body against loads. Secondly, the skin of the foot has no sebaceous glands, so that the hydrolipidic film is less rich in fatty components. Finally, this epidermis presents a large number of eccrine sweat glands, through which water, mineral salts and waste substances are excreted.8
The group of plantar receptors that provide the foot with sensitivity is heterogeneous due to the different types of skin receptors and the diversity of existing afferent nerve fibres.9 With the exception of nociceptors and thermoreceptors, most of the skin afferents correspond to the mechanoreceptors, which respond to pressure and vibration stimuli, and are related to myelinic afferent fibres (fast conducting fibres).10
Mechanoreceptors can be classified into two different groups: rapidly adapting and slowly adapting. Within the first group, we find Meissner’s corpuscles and those of Paccini.11 The former are also called tactile, and are located superficially (intervening in surface touch and responding to low-frequency vibrations).12,13 Paccini’s corpuscles are found in the deep dermis of the skin and the interior of the adipose plantar tissue and respond quickly to sensations of deep pressure, high frequency vibration and stretching.14
In addition, we can find two types of slowly adapting mechanoreceptors: Merkel’s disks and Ruffini’s corpuscles.15 Merkel’s disk is located on the surface of the epidermis of the skin and is involved in surface or discriminative touch. Ruffini’s corpuscles are considered to be a variant of Meissner’s corpuscles and are located more deeply, mediating sensations of thick and persistent touch.16
In addition, sensitivity levels on the plantar surface may vary greatly within the healthy17 and pathological population,18 with very different activation thresholds being observed depending on the age, area of the foot, sex or type of stimulus presented (vibratory or pressure-based).19 All this suggests that plantar afferent information could directly influence rebalancing ability and the creation of motor patterns.
Therefore, the main objective of this study is to analyse the influence of plantar sensitivity on changes in the ability to rebalance and manage movement, analysing the mechanisms that enable this to be assessed, and describing the factors that influence it.
Methodology
The different articles analysed in this study were located in the on-line computerised databases PubMed (Medline), Web of Science and SPORTdiscus. The keywords used for the search were: “sport injury”, “sensitivity”, “skin”, “foot”, and “posture”. The search terms were initially used independently and were subsequently grouped using the terms and and or. Regarding the selection criteria, we included experimental and quasi-experimental studies in English, published in impact journals. The search for articles was restricted to the period from January 2000 to January 2016. In addition, regarding the remaining inclusion criteria, the PICR (Participants, Intervention, Comparison, Results) reference was followed. The articles included were organised using “Mendeley” publication management software. Once the different studies had been analysed, duplicates were discarded; studies with little methodological rigueur; case studies; or those where the subject matter did not exactly fit our study objectives; and those whose text could not finally be obtained.
Results
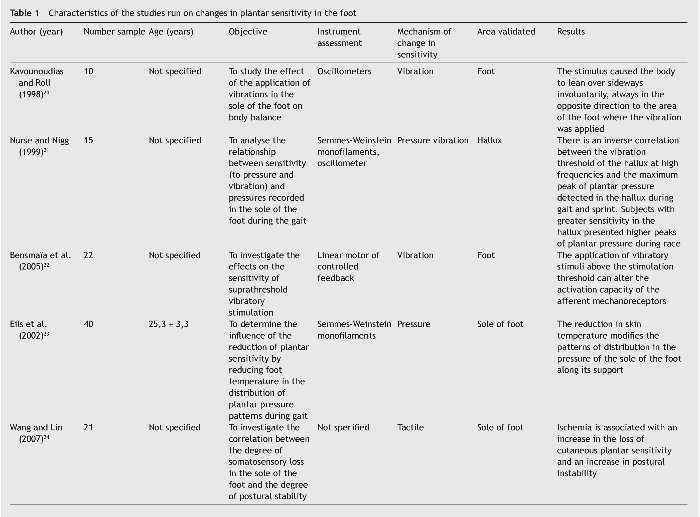
The article search and selection strategy adopted in this review obtained a total of 9 articles which finally met the inclusion criteria. The characteristics of the different studies identified can be found in Table 1.

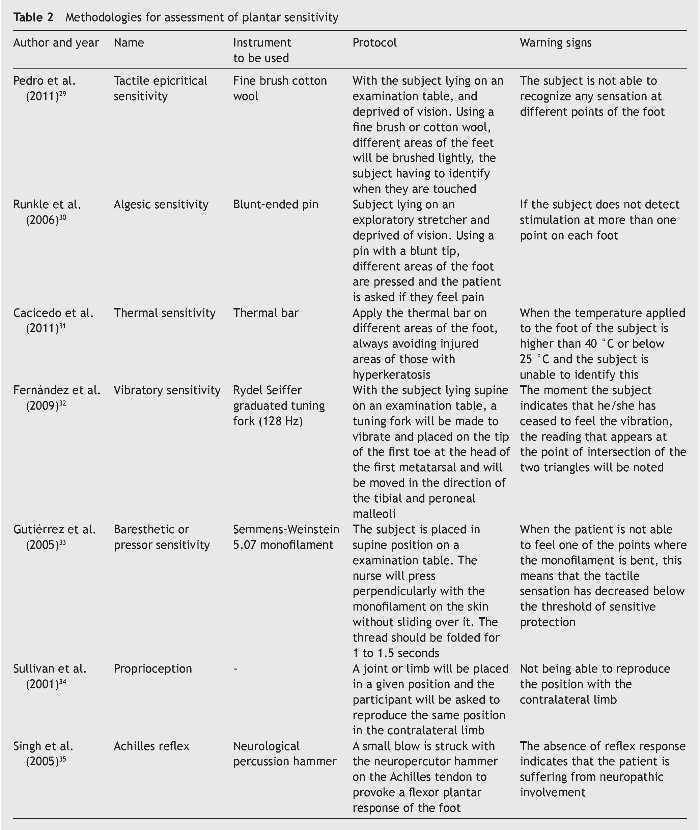
Several different methodologies have been used for the assessment of plantar sensitivity: tactile,29 algesic,30 thermal,31 vibratory,32 baresthetic,33 proprioception,34 reflex35 (Table 2). In general, in these methodologies, mechanical stimuli of different intensity are usually applied at symmetrical points on both hemispheres of the body, or the level of sensitivity between different body areas is compared.36 To achieve this, it appears to be important that the assessments are performed in the absence of fatigue, since it has been evidenced that the existence of fatigue seems to have a negative influence on assessment.37 Although many of these methodologies come from the clinical field,38 many can be applied directly or with slight modifications in healthy subjects and sportsmen.39
External factors influencing plantar sensitivity
Temperature
Several studies have suggested that the local application of cold seems to acutely increase sympathetic nervous activity in the applied area;40 to produce local reflex vasoconstriction;41 to reduce the skin temperature,42 and to alter local sensitivity.43 On this point, Nurse and Nigg6 found that the pressure centre moved from areas where cold was applied to areas where sensitivity was greater, and variations in patterns of muscle activity were recorded. On the other hand, Eils et al.,44 following a similar methodology, found reductions in the peaks of plantar pressure on stimulated areas and an alteration in plantar pressure patterns. This fact can be interpreted as a form of body protection, where the body attempts to avoid contact in areas of the foot where sensitivity is altered, seeking a support that searches for areas with greater sensitivity.
Footwear
Several authors have theorised about the influence that sport footwear could have on changes in plantar sensitivity as regards the information provided afferently from the plantar receptors45 and the reduction of their stimulation threshold.46 Factors such as hardness, design or thickness of the sole of the footwear,47 the type of footwear,48 the type of insole,49 and the use of certain specific footwear, such as football boots,50 appear to directly influence the level of plantar sensitivity. In addition, it has been shown that the use of air pocket footwear could increase the instability level in the foot and increase the risk of injury, as a result of the reduction in afferent information.51 It has also been seen that certain footwear, such as minimalist footwear, could also have repercussions on plantar sensitivity levels,52 especially when this provokes painful stimuli.53 On this point, it is clear that the type and characteristics of foot-wear used could produce changes in the quantity and quality of the information collected.54
Type of contact surface
The hardness of the terrain or footwear are factors that can affect plantar sensitivity and influence the pattern of movement.55 Chiang and Wu56 observed that as soil hardness reduced to a softer surface, body stability decreased, afferent response times increased, and plantar pressures recorded changed, all of which resulted from changes in skin receptors rather than muscle receptors.57
Hyperkeratosis
Hyperkeratosis occurs when there is thickening of the corneal layer of the epidermis caused by hypertrophy (enlargement of its cells) or hyperplasia (increase in the number of cells). This increase in the size or number of cells mainly affects the keratinocytes or corneocytes, which are the most numerous cells in the outermost layer of the epidermis.58 Plantar hyperkeratosis is able to inhibit sensory feedback in the area where it develops,59 which will cause displacement of the centre of pressures from the areas with less sensitivity to those with greater sensitivity.60
Mechanical vibrations
Although the vast majority of studies on the vibrotactile perception of the skin have been run on the hand, there is a high degree of consensus as to the influence that mechanical vibrations have on the foot, especially in certain pathologies such as the diabetic foot. This is due to the large number of mechanoreceptors present in the sole of the foot (Kennedy and Inglis61 located 104 mechanoreceptors in the skin of the human foot), and to the existence of specific vibration thresholds depending on the area of the foot (lower vibrotactile thresholds have been found in the midfoot than in the heel or toes).17 All this will affect the existence of specific efferent responses, depending on the type of vibratory stimulus presented. In this direction, the use of mechanical vibrations as a training method has been found to alter the level of plantar sensitivity and affect rebalancing ability,62 especially in the 10 min after its application and when mechanical vibrations are high frequency.63
Propioceptive insoles
It has recently been suggested that the placement of insoles of different textures seems to improve postural control,64 increasing the ankle’s ability for positional discrimination, preventing the appearance of injuries65 and creating more efficient muscle patterns.66 In addition, these improvements seem to appear in a relatively short time (5 weeks).64 Santos et al.67 found that the use of football boots decreased plantar sensitivity due to a reduction in the foot-ground contact area and an increase in plantar pressure peaks, and that when football boots were used in combination with stimulatory insoles, sensitivity and proprioceptive response improved considerably.
Discussion
Traditionally, the foot has been considered as a fundamental link within the maintenance of postural balance.68 The first models that attempted to explain how human beings rebalanced presented the body as an inverted pendulum69 whose axis of rotation was located in the ankle and where the constant wavering of the centre of gravity was readjusted, thanks to the information provided through afferent pathways.70 Although other explanatory models were later presented that attributed a fundamental role to the hip in the rebalancing process,71 at present there is a certain degree of consensus as to the existence of a combined and intermittent model where there is specific interaction between different body parts involved in a posture or movement.72 This will be configured, to a large extent, from the information provided by the somatosensory system.73
On this point it seems that the information provided by the plantar receptors is fundamental, since it seems that any alteration in the sensitivity of the skin receptors in the sole of the foot could have direct involvement in the alteration of the kinetic and muscular support patterns.74 For example, several studies have observed that, in subjects subjected to weightlessness, the loss of afferent information provided by the sole of the foot could lead to a decrease in the activity of the tonic muscles.75 Kozlovskaya et al.76 found that by submerging a group of subjects inside a tank of water for an extended period of time, there was a decrease in the activation levels of the extensional postural tonic muscles77 and an increase in those of the flexor,78 as a consequence of the removal of the afferent information provided by the sole of the foot. Although many of these changes are going to occur locally, all this suggests that changes could also be produced at the brain level.79 For example, Liepert et al.80 found that after 4-6 weeks of immobilisation of the foot as a consequence of a fracture, there was a decrease in cortical representation in the brain in the area corresponding to the foot.
Similarly, it appears that a decrease in sensory feedback levels in selective areas of the foot during gait could cause displacement of the centre of plantar pressure from areas where there is a loss of sensitivity to areas of the sole of the foot with greater sensitivity.81 This may produce changes in plantar pressure patterns (peak pressure and pressure-time integral). Moreover, it seems that all this could have repercussions on the muscles involved in the movement and their level of activity.82
On the contrary, several studies suggest that certain activities may favour the local ability to collect afferent information or the central ability to activate specific brain areas, generating specific adaptations resulting from training. Meier et al.79 found that, when comparing professional handball players with professional dancers, the latter were able to optimise the level of activation of specific areas of the brain related to segmentary control of the foot. This could be due, at least in part, to the development of a greater sensory ability developed in the dancers, due to working barefoot, adopting different positions on the foot in situations of instability and stimulating very reduced areas of contact. Similarly, there have also been improvements in levels of brain activation in athletes who use their feet specifically in their sports. In a study comparing the football player, Neymar Jr., with other football players (three professionals and one amateur) and two professional swimmers, it was observed that Neymar had less neural activity in the area of his brain related to the foot when making simple movements with it, which was interpreted as a sign of efficiency.83 In addition, these results are in line with those obtained in other bodily regions such as hands, in groups that usually have to develop high levels of performance, such as pianists or keyboard players.84 This has also been observed in primates.85
All of this suggests that any alteration of the information provided afferently from the feet could modify the patterns of muscle activation during standing,41 directly influencing postural stability levels.
On the other hand, several studies have shown the existence of a direct relationship between a decrease in plantar sensitivity and increased risk of lesion. For example, it has been observed that sportsmen who have suffered ankle injuries have lower levels of postural stability,86 a decrease in joint stability levels, and altered motor patterns.87 Similarly, Steinberg et al.88 observed that in patients with anterior cruciate ligament injury there was poorer vibratory sensitivity in the foot and ankle.
These changes appear to be the result of the appearance of a change in the functioning of the afferent information channels, provoked by the lesion, which justifies the need to re-educate and optimise its functioning. On the other hand, the possible negative influence that cryotherapy (as a treatment or recovery method) may have on proprioceptive ability has been questioned, verifying that the effects on proprioceptive ability may be variable, depending on the time of application89 and the body area analysed.90
Several authors have researched the effect of proprioceptive ankle training on static body balance, noting that in healthy individuals, this produces positive effects.91 Han et al.92 measured the ankle’s proprioceptive ability in 100 elite athletes from 5 different sports (gymnastics, football, swimming, badminton and dance), observing a direct relationship between the level of ankle proprioception and performance in sport, even at Olympic level. All this appears to indicate how obtaining improvements in body balance through plantar sensitivity enables sportsmen to reduce the level of attention they have to pay, consciously or unconsciously, to the maintenance of stability, thus being able to devote more attention to improvement in their technique. In a study comparing gymnasts with sportsmen who did not specifically work on proprioception, it was observed that the former decreased their dependence on postural control processes when they were subjected to different tasks or tasks of greater complexity.93 Therefore, it seems logical to think that specific training of plantar receptors could have positive effects on creating and optimising motor patterns. Improvement in this regard should therefore be considered in both sport and preventive and injury treatment programmes.
Conclusions and recommendations
As suggested by our review, sensory feedback from the foot is essential in the maintenance of general (postural and displacement) and specific (sport) patterns. Changes in the quantity or quality of plantar afferent information will not only upset the creation of different patterns but may also increase the risk of injury. In this sense, it will be fundamental to maintain and optimise the ability to collect afferent information from the different systems, as a way to avoid the appearance of injuries and pathologies and improve performance. Continuous monitoring of information gathering levels, coupled with the creation of stimulation tasks, are alternatives that should be considered.
Conflict of interest
The authors declare no conflict of interest.
Received 28 April 2016;
accepted 12 September 2016
* Corresponding author.
E-mail address: calebaraguas@hotmail.com (C. Araguas Garcia).

