











The objective of this study is to describe the relationship between injury incidence (IL) and maturity in male elite handball's player (HbP). Prospective study during two seasons, evaluating the sports injuries, maturity status and exposure time in hours in 133 young handball's players, under the UEFA methodology model for epidemiological studies. We discuss the maturity stage with different parameters, the Tanner's stage, puberty stages, peak high velocity, testicular volume, and the bone age. Finally, 190 injuries for a total of 34.222 h of exposure were registered.
The average total Injury Incidence (IIn) by categories was 5,6 injury/1000 h of exposure. Injury Incidence during competition: 21,8 injuries/1000 hs and in training: 3,1 injuries/1000 hs without statistically significant between IIn, chronological age and different maturity stage by ANOVA.
The multivariate statistical analysis registers tendency associations between IIn in competition for category (P = 0,07), and the IIn in training for Tanner stage (P = 0,091) and puberty (P = 0,021).
In conclusion: there is not a significant difference in total IIn by ages categories in handball players but there is statistically significance tendency respect to some maturity parameters under a multivariate analysis. This last result must be considered when planning training seasons and strategies for injury prevention in the context of the formative handball.
Handball is one of the most popular sports in Europe and Spain.1 Although healthy,2 after football is the team sport with a higher injury risk3-5 In order to understand the characteristics of the injuries and stablish prevention tools, epidemiologic studies are considered basic, mainly during the maturation process.3-6
Puberty is the last transition period between childhood and adult stage. It begins with a sequence of maturity changes, leaded by neuroendocrine and hormonal factors, under the environmental and genetic influence, and enhance the growth and the appearance of secondary sexual characteristics.7,8 These ones are evaluated with Tanner staging criteria (sexual secondary character) and the measure of the testicular volume in males.9,10 Otherwise, another aspects regarding with the growth are measured by the peak height velocity (PHV), which appears in the middle of puberty, after a significant exposure to androgen (mean testicular volume of 12 ml and Tanner 3 to 4).11 In this respect, most of the studies about maturity and sports consider the bone age as normal value when the difference with the chronological age is the same or less than one year.10 All these parameters may help to determine the maturity status, which have a strong influence in performance and by extension in the profile of injuries.
The aim of this study is to describe the relationship between the maturity stage by different methods and the Injury Incidence (IIn) in a group of high-performance youth handball players (HbP) regarding the different category-age.
Material and methodsFrameMale handball players in a south European sport club were followed up. The different team categories-age of this club were regularly in the top 3 of the national competition at the moment to collect this data. All the players in each team for this club were selected for the national team elite program, due to their high individual performance.
ParticipantsThe handball section in this club was composed of 203 players. First team players were excluded from the study, the remaining 164 which were elected using the inclusion and exclusion criteria shown in Table 1.
Inclusion and Exclusion criteria of the first and second research stage.
*Note: The general criteria (1st stage) determine the maturity criteria (2nd stage).
A follow up of 5 team categories: U14, U16A, U16B, U18 and Senior B. As the study was done over 2 years, we considered 10 teams, analyzing team and player by season obtaining a total number of 164 subjects. The first team adult players were excluded, as they have a more intensive competition program, with two matches per week. The adult players were recruited from the second team (Senior B), which competes once a week as same schedule as youth categories. Despite the fact all teams are considered for developing handball players, due to the age and maturity status, we considered categories U14 to U18 still in development and Senior B (>18) team as control group.
DesignAccording to standardized STROBE criteria, the current research is a prospective, longitudinal descriptive and observational study, along 2 consecutive seasons. All players signed the written information consent as a routine protocol in the club, in concordance with Declaration of Helsinki. This study was approved by the Research Ethic Committee of the Consell Català de l'Esport.(NO 00995/5954/2013)
The inclusion and exclusion criteria is described in Table 1, and the flowchart inclusion participants in Fig. 1. IIn was analyzed in 164 players-season of different ages and categories, and 133 (<18 yo) of them were tested at least once, for the maturity stage in the following parameters: Testicular Volume (TV), Tanner Genital stage -secondary sexual characters- (T), puberty (P) and the changes of these parameters during the season considered the tempo during the maturation process. Those values were expressed at incremental outcomes named: delta T and delta TV. Additional parameters as PHV and Bone Age were assessed during one season in 65 players.
Planning and procedure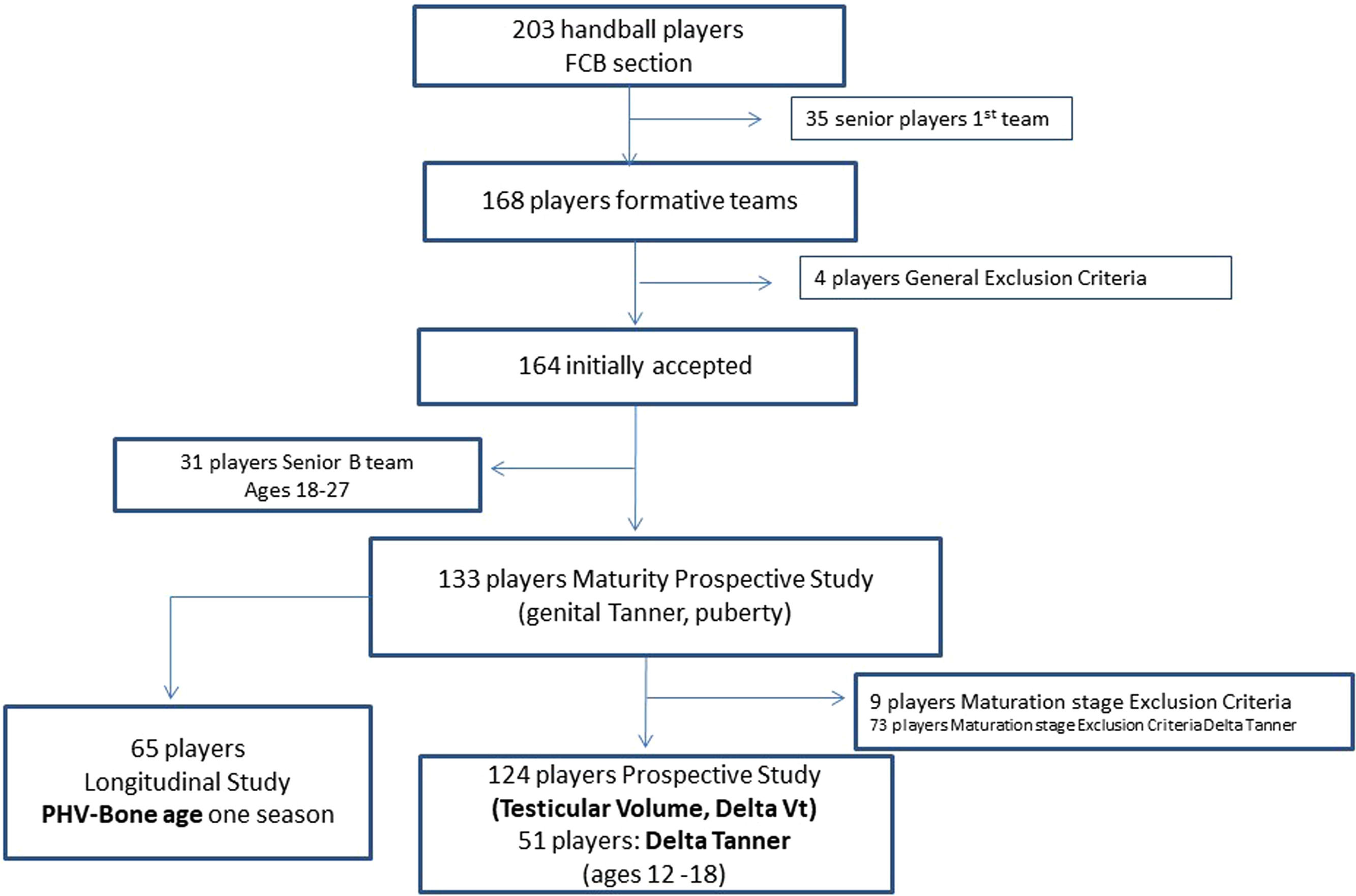
The study was done during seasons 2011–12 and 2012–13. All the HbP had medical screening at the beginning of the season, and the follow up of the variables collecting in the screening according to the guidelines of the institution. 12,13
Each season is shown in quarters: 1st August-September-October, 2nd November-December-January and 3rd February-March-April. In May the competition is over, with a holidays period from June to July. The maturity assessment (TV, T, P) was done at the end of the first and third quarter (Fig. 2.) The PHV was assessed considering both measurement of height and their increment; and bone age was performed in the first quarter of the season period.
Study of injuries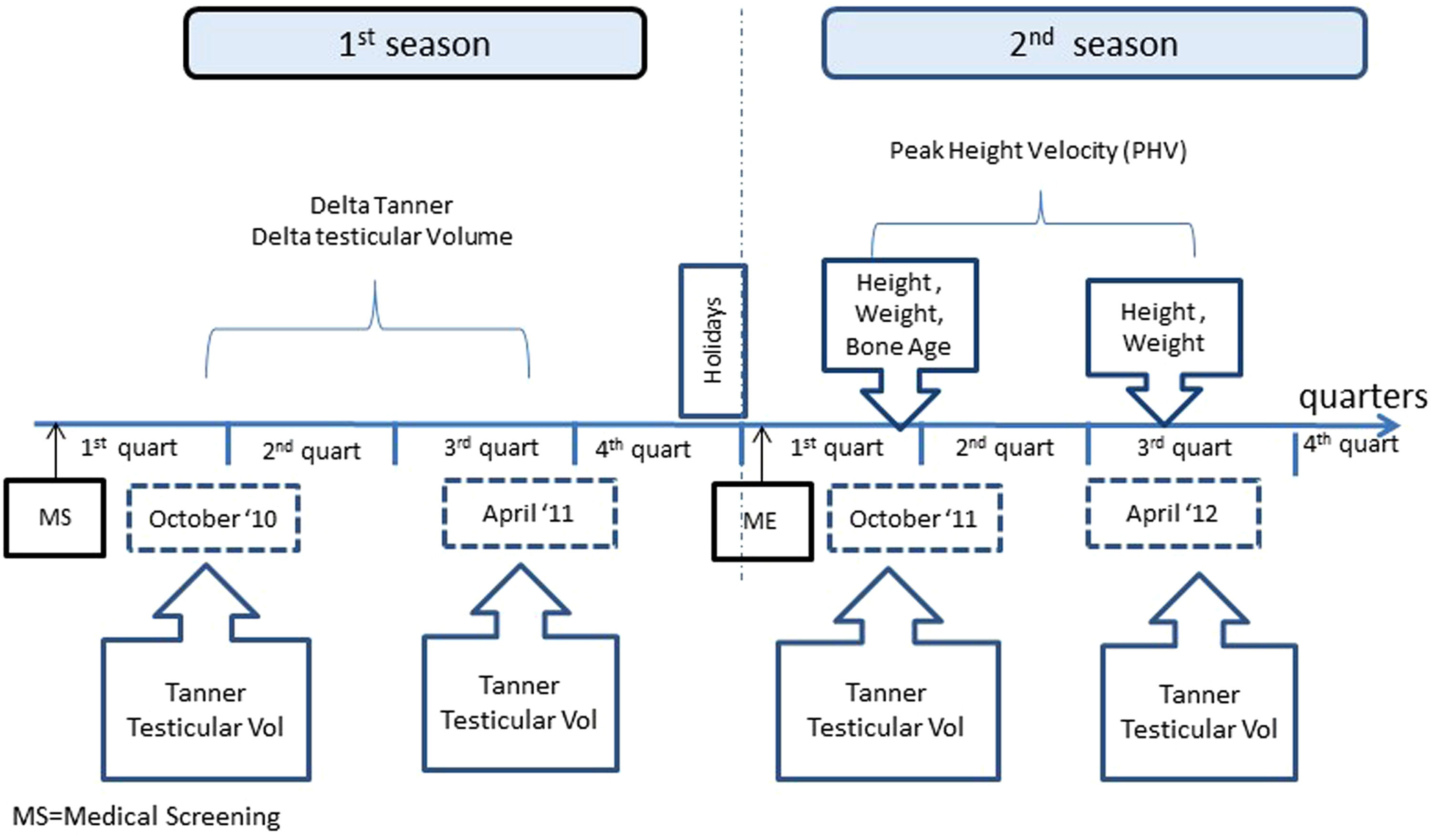
Diagnoses and records of injuries were done by the same staff, composed by two sport medicine physicians, with more than 20 years of experience in Orthopedics and Handball medicine, one of them also is pediatric specialist (JAG y MM). Moreover, the injuries criteria followed the definition and recommendation for epidemiological injury studies provided by UEFA.14-16
The injuries were categorized regarding the time loss, sport condition, training, or competition. A category of Unknown was defined for insidious injuries, in which the player was not able to define the origin of the injury during the 12 h after the last sport practice. The hours of practice exposure were registered for the coaching staff.
Maturity stageThe maturity assessment was performed twice a season, in the same month and at the same timeframe each year (October and April), with 6 months difference between them.
All the parameters were measured in one single day (afternoon), for the same pediatrician, to avoid the seasonal and interobserver variability, except for the bone age values (once). The day of assessment the training was canceled, and 48 h before it, the workload training was reduced.
Main outcomesWeigh, height, and body mass index (BMI) were measured according to previous researchers 17 and the maturity stage following previous authors recommendations18-20
Direct outcomes- -
Testicular Volume (TV): it is defined as the size in ml, measured in comparison with Prader orchidometer. The player remains standing, in front of the evaluator, which palpates the testicle before and after Valsalva maneuver to rule out testicular disease.
- -
Tanner stage (T): is the genital aspect of the Tanner stage (G1-G5), evaluated by visual inspection by clinician.
- -
Bone Age (BA): Tanner Whitehouse III (TWIII) method was used, with x-ray of left hand. The reading BA used an automatized bone age software (BoneXpert®) externally by experienced clinician to avoid variability interobserver. Usual outcomes of BA were defined: TWIII–Chronological age. If BA <1 retarded or slow maturation; value as 1 normal and >1 BA advanced or early maturation.21
- -
Puberty: it was grouping the TV values into an establish range, regarding the pubertal period (No significant differences were found between subjects with or without testicular disease)
- ○
Prepubertal or P1 = TV 1–3
- ○
Initial Puberty or P2 = TV 4–6
- ○
Mid-stage puberty or P3 = TV 8–12
- ○
End of Puberty - final stage- or P4 = TV 15–25
- ○
- -
Delta Tanner (Delta T) or tempo is the difference between the value of second and first genital Tanner assessment during same season. The dynamic nature of the maturity stage was evaluated, as well as the progression in maturity of the subjects during the observed frame time.
- -
Delta Testicular Volume (Delta TV): is the tempo or variation between second and first TV assessment.
- -
PHV: height increased in centimeter (4–6 cm) in 6 months period, which it suggests an increase of 8–12 cm/year.
The devices used for the measurements for weight and height were a scale Tanita WB-3000plus (Tokyo, Japan) precision 0,1 kg and stadiometer Harpenden (Crosswell, Crymych, Pembs, UK) precision 1 mm. The X-ray system used to evaluate hand palm and carpus was Carestream DRXEvolution (Salt Lake City, UT, EEUU) device and a software to read automatized bone age (BoneXpert ®). Measurement of TV was performed using a Prader orchidometer (Holtain Prader Crymych UK Ltd).
Statistical analysisThe IIn, defined as the number of injuries per 1000 h of exposure, was analyzed using multivariance statistical methods, applying the statistic software SPSS 13.0 for Windows. At the same time, it was performed an analysis of variance to calculate the influence of maturity outcomes, for Tanner and Puberty. Moreover, a multiple analysis of variance was conducted to analyze the influence of the same maturity outcomes over the IIn.
ResultsTable 2 shows the general descriptive data of the sample, mean and standard deviation of age, weight, height, and BMI.
General description data.
Note: BMI (Body mass index); SD (standard deviation).
A total of 190 sport injuries were registered, considering more than 1 day of sport nonattendance (Table 3). The hours of exposure were 34.222, with a larger amount of training hours than competition. Competition IIn is higher than in trainings. The total mean of IIn was 5,6, divided into 21,8 in matches and 3,1 in trainings.
Descriptive data about injury incidence by age and team/category.
The hour of exposure is different between category teams. The U14 teams have less exposure time, and Senior B the highest exposure time but the frequency of games per week is the same.
The larger peak of IIn was observed at the age of 17 (8,1), followed by 12 and 13 years (6,6 and 6,2 respectively). IIn regarding the age and category is showed in Table 3, without statistical significance between the different outcomes.
Table 4 presents IIn in relationship with the maturity parameters. One finding is that most of the sample were at the end of the maturity process (61 % in Tanner 5, 37 % 2 to 4, period with the most significant changes, and 0,9 % Prepuberal stage). No significant statistical difference was found in IIn between maturity groups. The BA describes 66 % (n:43) are in normal status of biological bone age, while 15 % (n:10) shows slow maturation and 17 % advanced (n:11) and one data was missed.
Total and partial injury incidence, regarding training or competition during 2 seasons and maturity stage.
Note: SD (Standard Deviation).
The normal evolution of maturation is seen with the concept of tempo when the change from one Tanner stage to another (Delta Tanner) is done. For that reason, the players with Tanner 5 were excluded after the first assessment at beginning of the season, remaining a total of 51 players, 4 of them not were able to do the second medical evaluation for unknown reasons. The mean age of this group (Delta Tanner) is 13,7 years, (SD 0,9), and 59 % of them (n = 30) changed their stage at least in 1 point (IIn 6,5), while the remaining 41 % without changes (Delta Tanner 0) showed an IIn of 4,3, with no significant statistical differences.
Testicular volume analysis showed all participants started the puberal changes at the beginning of the study (TV ≥ 4). Moreover, the measurement allowed to group the sample according to the TV in the Puberty outcome, which is a useful way to group the parameters for a further analysis when we study small sample.
Puberty outcome was performed in a total of 133 players. A 75 % of population is mature or in a end of puberty stage, according to this classification and 25 % was still in a growing development period. According to this outcome, the highest IIn was found during initial puberty, without statistical significance.
The changes on testicular size during a season (Delta TV), 46 % didn't have changes on testicular volume (n:57) and 47 % (n 58) increased size between 3 and 13 ml without statistical significance even when the volume was grouped by Tanner stage (Table 4)
The analysis of PHV (n:65, one data was missed) shows that 11 % (n:7) of the players had a higher increase in height (cm/year). A similar number of subjects did not show any increase in height (17 % n:11), 9 % (n:6) 0.4 cm and 61 % (n:40) with a minimum increase 0,5 to 3 cm in height. Mean age was 15 years (SD 1). The relationship between IIn and PHV did not show statistical significance.
Finally, multivariance analysis of the IIn as per category-age, Tanner, TV and Puberty only found significative differences between IIn in competition between category and IIn during training for Tanner and Puberty variables. No significant differences in the rest of parameters were observed (Table 5).
Multivariate analysis. Statistical significance of the injury incidence in relationship with category and maturity stage (by Tanner, Testicular Volume and Puberty).
NS= No statistical significance.
VT= volume of testicles.
The main finding in our study is that IIn in youth Handball players don't show significant difference according to chronological age with the same model of individualized game/training. However, if the IIn is analyzed concerning maturity stratus, it shows some differences. In our knowledge, this was the first study series to describe some correlation between maturity stage and injury in handball.
Injury incidenceInjury incidence in some sports have been related with a higher chronological age22, however in handball studies there are some differences regarding the age5,23 and other study determine the years of practice as a unique factor with more numbers of injuries24.
Differences in maturation status between players produce an inequality condition for competition and influence for risk of injuries.21,22
Some authors studied the relationship between secondary sexual characteristics and injuries in football25,26 but not all of them studied the risk of exposure, therefore this limitation may condition the conclusions.27
The current prospective study over 2 consecutive seasons, was designed to minimize the risk of bias due to the bimodal curve of the IIn between seasons in sport teams. Moreover, we should consider the extra amount of load for some subjects who participate in national team competition, but this complementary information has not been considered, as in other studies. 14 Sample size was delimited to males, to avoid bias in gender. 28,29 As we mentioned before, height, weight and BMI experience an increase along the years due to maturity and all the subjects have a standard deviation higher than the Spanish general population for a natural selection for this sport.17,30 The singularity of this sample, limit the option to link our conclusions to general population or others handball academies, unless for subjects with similar characteristics and model of training.
Recent review conducted by Raya-González et al.31 about the IIn in handball shown that senior male handball players showed the highest value (7,8 injuries/h exposure), while lower incidences were observed in male youth players (6,9 injuries/h exposure). These data are slightly higher compared with the senior team (6,1 injuries/h exposure) in our study but are the same for our U14 group. As long as the reviewer considers included in senior category not only league competition but also international competitions, which an increase in the number of matches could explain the differences in the results. In general, IIn in competition is higher than in training, as previous research found.28,32 It must be considered in our study, the hours of exposition were estimated regarding the category. Analyzing IIn in competition in relationship with the category lead to a decrease in the risk of mistakes, compared with the use of the maturity outcomes. Moreover, competition injuries depend on contact exposure and mechanism, so an advanced maturity stage could be considered as an advantage against the opponents in youth HbP. The inclusion of Senior B team in the analysis per category, a semiprofessional team since 2 seasons ago, implies a higher level of exigence and therefore an increase of IIn in competition in comparison with the rest of the teams. Currently, Senior B and U14 present a total IIn higher than in previous seasons for same club5. These differences regarding the previous seasons in some team-categories are related to the study design were some players forward to next team category in consecutive seasons, some changes in the model of training, or that the Senior B increased to a highest level of competition (second division) at the beginning of the study. We chose the Senior B, instead of first team, as control group (for to be considered adult) because they plays at highest level division for adult category with one game a week with same frequency than the rest of others categories to avoid bias.
Likewise, we must keep in mind that in U14 teams, some of the players are selected despite their low maturity stage, focused on the long-term development athlete program instead of results in competitions at this technical stage 5
Maturity assessmentMost of the research on this topic are focused on parameters as BA or maturity offset, somatic (percentage of adult height prediction, estimated PHV by equation or assessment, etc.),38,39,40,41 but not studies were focused on secondary sexual characteristics, and none study was conducted in handball before this series. The assessment of maturation, for daily practice could be divided in three periods, prepuberal, puberty changes and end-puberty, with independence of the method used (somatic or Secondary sexual characteristics), but the Tanner stage is the gold standard to assess puberty. It's the earliest to identify the onset of puberty before any other somatic changes as PHV or growth spurt is done, given complementary information of health.37
In this research, a 100 % of the sample size already started their puberty at the beginning of the study (TV ≥ 4 ml), showing most of them already reached final stages of maturity; Tanner 5: 61 % (n: 82), TV >15: 70 % (n: 92) and final Puberty 76 % (n:101). Like that, data shows around 25 %−40 % of the sample are in a period with a high percentage of some development changes.
The rapid growth has been associated with increased risk of injuries.41,42 This dynamic process of maturation is seem analyzing the variables of tempo, as Delta Tanner, Delta TV and PHV. Those didn't show significant differences between subjects who experienced changes or not during the season as also was described by LeGall.33
The advanced maturity status of the participants, age and sex probably predisposed a data with higher values than in normal population.34 We don't know if this fact is related to natural selection process for this sport or the practice of handball lead to a faster advanced maturity stage, in any case none of them were in abnormal range. 10
Correlation between injury -maturity stagePrevious studies show that subjects in a final stage, as Tanner 5, are likely to have a larger total IIn25,26,35. However, these results are different from our findings, probably due to the specificity of the sport, the elite profile and singularity of this sample (maturity status included). This last aspect would require further investigations with a larger sample size with more players in the prepuberal or early puberty stage. We must highlight that most of the previous studies were done in football, with less contact sport and different skills-demands, but none of them studied the secondary sex characteristics and somatic parameters (PHV) and BA at same time.25,26,34,43
Assuming the minimum age in our research is 12 years, we cannot indicate the moment to initiate puberty and in consequence the onset of normal puberty. For that, we examined the BA to point out the normal population and the IIn in relationship with the stage of early, normal, or advanced maturity. So far, the maturity offset of 1 year difference between chronological vs bone age showed no significate differences with IIn. At the moment to submit this manuscript, a recent study was published questioning this categorization for lack of consistency in the results and probably the optimal value could be more than 1,5 instead of 1 year difference between them. For this kind of analysis, a bigger sample of subjects would be need it.34,35
Previous research reports that later adolescence (T:5), and advanced bone age are linked with higher rate of IIn.25,26 In this study, our results agree with previous research, in terms of high IIn in early or advanced BA (but without statistical significance). However, our data differ between IIn and sexual maturity (without statistical significance) in comparison with the literature above mentioned. 25,26
Puberty outcome shows the most relevant period of maturity changes (P3) is correlated with a higher IIn during training, using a multivariance statistical analysis. It could indicate the players in an intermediate puberty stage when we expected the more important somatic and hormonal changes are more likely to be injured during a training.
Non statistical significance was found between IIn and maturity, probably conditioned by the physical demands by player position, the nature of this sport and the small sample. Similar results have been found in previous research, with a high risk of bias and a non-clear association between maturity status and higher injury incidence as a main result in previous study conducted36. In youth handball, players with advanced maturity stage use to play in the positions demands a higher physical contact. This fact could explain the differences between IIn in Maturity-Training and between Categories-Competition.
The multivariance analysis of IIn shows correlation in Competition and Categories (P = 0,07) and for Training with maturity variables as Tanner (P = 0,091) and Puberty (P = 0,021) outcomes. These previous results are statistically significant or a close trend to be, while in the rest of parameters we didn't find significance or statistical trend. Perhaps with a bigger sample, this trend could be clearer. The main finding in the current study is the higher IIn in training regarding maturity outcomes.
The contribution of this manuscript is the use of sexual secondary characteristics for the assessment of maturation status. The traditional Tanner Stage criteria (genital and pubic hair) and testicular size was assessed by an experienced pediatrician. We are aware that most of the clubs and academies don't have pediatrician or physician to complete this kind of assessment, but most of the pediatric population have access to a primary care center where their doctor of reference may contribute to provide this information for sports science if it is need it.
The analysis of different maturity parameters we contribute to using the Puberty classification that we grouped players according to the size of testicular volume according to the puberty period related with somatic changes. This classification probably is better to identify maturation changes respect other parameters when the sample is small.
The authors consider that probably the profile of injuries and not only the injury incidence could be more useful for daily practice to prevent injuries in handball academy.
ConclusionsNo significant differences were found between total IIn and chronologic age, neither IIn or the different maturity stages, after have been analyzed with ANOVA. However, the multivariance analysis seems to find a correlational trend between IIn in Competition and Categories, and between Training with maturity stage. This fact suggests, in the case of a larger sample size and frame time of a similar study, the results could have a stringer statistic significant.
Practical applicationsThe maturity parameters are more specific than chronological age to be considered in the training periodization as well as in the injury prevention programs in Handball.
Identifying the maturation status may help to individualize the training in youth and probably to reduce the impact of injuries but we shouldn't consider it a risk factor by itself as a single factor.
The model of training and workload, and not the maturation changes isolated are probably the risk factor for injuries in youth athlete.
Another practical application could be the addition of the maturity assessment during annual medical screening, as tool to categorize the player, plus to rule out medical conditions.37,38
The use of puberty classification by testicular volume size could be an alternative option with small sample size.
Research about maturity and injuries can vary by sports and/or training model.
Limitation of the studyThe main limitation for this study was the advanced maturity stage in most of the players at the beginning of the study, due to natural selection in handball for mature players.
A larger sample size, with more players in prepuberal stage or early puberty stage is needed in further investigation to see clear association with injury incidence, but the nature and singularity of the sample conditioned us in this aspect.
Future perspectivesFurther investigations should analyze the different injury patterns, burden, and severity of the injuries in relation to maturity outcomes, player position and model of training. Furthers studies involving early puberty stages and burden of injury, could be beneficial to design prevention strategies in elite and amateurs handball players or other sports.
Note of authorsThis article was published in Spanish version at same journal.
Regarding the interest of many colleagues for an English version we submit the current original version with mild modifications and updated literature.
FundingThe study did not receive any external funding.
To all FCBarcelona staff at the moment to collect the data, Toni Gerona and coaches in FC Barcelona youth Handball, due to registration of the exposition hours and collaboration. Ramon Navarro, PT of Handball Academy.
Mrs. Joan Manel García & Xavier Fernández PT & NP for the excellent management of the agenda, performance of X-ray and measurement of anthropometrics parameters at the moment to collect the data.
The co-autors of first version of this manuscript, Joan Nardi Vilardaga, Lluis Til Pérez, Franchek Drobnic, and Carles Pedret Carballido.

