






Balance of strength and flexibility between the dominant (DL) and non-dominant limbs (NDL) in young soccer players is essential, since it can minimize the possible injury-triggering mechanisms and their negative influence on performance. The aim of this study was to evaluate and compare the unilateral and bilateral strength and flexibility between the DL and NDL in young soccer players.
Material and methodsThe sample consisted of 30 individuals (aged 15.97±0.67 years). The isokinetic strength was measured at the velocities of 60°s and 180°s in the concentric action of the quadriceps and hamstrings as well as eccentric of the hamstrings, and in the conventional and functional ratios, along with hip flexion range of motion.
ResultsThe results showed the athletes had an eccentric strength of the hamstrings at 60°s in the DL significantly (p<0.05) stronger than in the NDL, and the DL had a significant H/Q ratio (p<0.05) more balanced than the NDL.
ConclusionsYoung soccer athletes may present a non-standard isokinetic results. These results are observed because of the difference in muscle strength of the posterior thigh compared to DL and NDL and the balance relation between the quadriceps and the hamstrings, generating an asymmetry of strength between the limbs and on the same member. It is necessary to monitor and devise training strategies to avoid these imbalances in order to prevent injuries.
El equilibrio de la fuerza y de la flexibilidad entre las piernas dominantes (PD) y no dominantes (PND) en jóvenes jugadores de fútbol es imprescindible, pues puede minimizar los posibles mecanismos desencadenantes de lesiones y su influencia negativa en el desempeño. El objetivo de este estudio fue evaluar y comparar la fuerza y la flexibilidad uni y bilateral entre las PD y PND en jóvenes jugadores de fútbol.
Material y métodosLa muestra fue compuesta por 30 individuos (con edad entre 15,97±0,67 años). Se evaluó la fuerza isocinética a las velocidades de 60°/s y 180°/s en la acción concéntrica del cuádriceps e isquiotibiales y excéntrica de los isquiotibiales, y en las razones convencional y funcional, además de la goniometría para la flexión de cadera.
ResultadosLos resultados demostraron que los atletas poseían una acción excéntrica de los isquiotibiales en 60°/s en las PD significativamente (p<0,05) más fuerte que en las PND, además de las PD tener una relación I/Q significativamente (p<0,05) más equilibrada que las PND.
ConclusionesLos atletas jóvenes de fútbol pueden presentar resultados isocinéticos no estandarizados. Estos resultados se observan debido a la diferencia en la fuerza muscular del muslo posterior con relación a las PD y PND y la relación de equilibrio entre el cuádriceps y los isquiotibiales, generando una asimetría de fuerza entre los miembros y en el mismo miembro. Es necesario monitorear y elaborar estrategias de entrenamiento para evitar estos desequilibrios, a fin de evitar lesiones.
Soccer requires a variety of physical valences such as muscle strength and flexibility, predominantly of the lower limbs. Among the main muscles of this segment are the quadriceps with an important role in kicks, passes, and jumps, and the hamstrings that help stabilize the knee.1 The relationship of these two muscle groups (agonist/antagonist relationship) is essential for the practice of soccer, since the balance of strength and flexibility between the dominant (DL) and non-dominant (NDL) limbs provides joint stability.2 Therefore, if one of these muscles does not perform its function correctly, a muscle imbalance occurs and may become a potential mechanism for the increase of injuries.3
Most soccer players use predominantly one limb and this may cause an imbalance of strength and flexibility between legs.4 Bilateral asymmetries between DL and NDL are related to a higher risk for injuries in the lower limbs and still appear to have a negative influence on the performance of athletes.5 In order to assess the strength and muscular balance, and consequently the presence of an asymmetry between the limbs, an isokinetic test can be used. Through these tests, it is possible to quantify the peak torque values (PT), work, and power of the quadriceps and hamstrings.6 In addition to the hamstrings to quadriceps ratio (H:Q), it is possible to obtain the values for the conventional ratio (concentric hamstrings PT/concentric quadriceps PT) and functional ratio (eccentric hamstring PT/concentric quadriceps PT).
Rahnama et al.4 reported the muscular strength of the knee flexors in NDL was greater than that of DL in more than 68% of amateur players in English soccer. Fousekis et al.7 found professional players with asymmetry in the eccentric strength of the hamstrings, suggesting an increased risk of these individuals developing an injury in this region. Daneshjoo et al.2 evaluating young professional players found that physical performance and pattern of movement experienced during soccer can negatively alter the balance of strength in both legs (bilateral strength balance). In contrast, Silva et al.5 assessing U-20 players did not observe significant differences in PT, or functional and conventional ratios between DL and NDL. In addition, Bonetti et al.8 investigating young players found DL significantly stronger for concentric action of the hamstrings and more balanced for the conventional ratio than the NDL.
Another important physical attribute to be evaluated is flexibility, which can be measured by the level of amplitude of movement of a particular joint, using the technique of goniometry.9 It can seen in the literature that athletes with a high degree of flexibility traditionally have a better movement proficiency, while the existence of asymmetry of flexibility between the limbs is an important risk factor for injury risk.2 Rahnama et al.4 did not report significant differences in flexibility of the hip joint between DL and NDL of soccer players. Fousekis et al.7 observed that only the asymmetry of flexibility would not be a potential factor for the appearance of injuries in players; however, when associated with an asymmetry of the quadriceps eccentric force, it is suggested a greater risk of injury in this muscle group. Daneshjoo et al.2 found greater flexibility of the hip joint in DL than in comparison to NDL in professional players.
It is noteworthy that young athletes are even more exposed to injuries and are in the stage of incomplete maturation and growth.3,10 In addition, the injury risk is multifactorial, such that when an individual presenting a flexibility imbalance combined with an strength asymmetry may further increase the possibility of injury.11 The assessment of imbalances could decrease incidence of these injuries, serving as a tool to detect and compensate for possible disproportions in the early life of training of these young athletes.12 Thus, the aim of this study is to assess the strength, through isokinetic testing, and flexibility, through goniometry, between DL and NDL in young soccer players.
Material and methodsParticipantsThe sample consisted of 30 men aged 15.97±0.67 years, body mass of 66.49±5.94kg, stature of 175±0.7cm, body fat percentage (Yuhasz Protocol) of 9.51±1.22%, and BMI of 21.69±1.32, athletes of the category U-17 of the Club de Regatas Vasco da Gama (Table 1).
The inclusion criteria considered were: (a) to be an apparently-healthy individual; (b) to be an athlete of the U-17 category; (c) be an athlete for at least three years; (d) have already participated in any official competition; (e) be in the period of preparation for some competition. Exclusion criteria were: (a) have a history of anterior cruciate ligament (ACL) injury or other knee or lower limb pathology; (b) to be relieved of his sports activities in the last three months because of injury.
The parents/responsible for volunteers who participated in the study signed the Term of Free and Informed Consent. The present study was approved by the Research Ethics Committee of the Federal University of Rio de Janeiro, under number 34315478.7.0000.5257, according to Resolution 196/96 of the Brazilian National Health Council, in addition to following the criteria of the Helsinki Declaration.13
ProceduresTesting was performed in the morning in an air-conditioned room where the temperature remained between 23 and 24°C. All tests were carried out by the same evaluators.
Anthropometric evaluationMeasurement of body mass and stature was performed through the use of a scale (Welmy Class III, Brazil, 2014); tricipital, subscapular, supra iliac, abdominal, thigh and pectoral skin folds with skinfold calipers (Lange Skinfold Caliper, Beta Technology, USA, 2008). Body fat percentage was calculated using the Yuhasz protocol.14 Body mass index (BMI) was calculated using the following equation, BMI=body mass (kg)/stature (m)2.
Flexibility evaluationUnilateral flexibility was measured through the use of goniometry of DL and NDL. The DL was defined as the limb an athlete preferentially uses to kick. For a warm-up, the athletes were instructed to perform two sets of static stretching, remaining in the position where they felt a mild discomfort for 10s in each repetition. After completing the first set, the athlete rested for 10s before performing the second set. Four stretching exercises were performed during this warm-up: (1) the individual in a seated position with knees extended, trunk flexed while leading his hands reached toward the feet; (2) the individual would support the knee on the mat and the other leg went forward supporting the foot on the ground, such that he leaned forward as far as he could; (3) the individual standing, flexing the knee, pulling the leg toward the gluteus; (4) the individual with his hands on the floor, front leg with knee flexed and foot supported on the floor, extended the back leg trying to put the heel on the floor.
After warm-up. the athletes laid in a dorsal position and with knees extended, the goniometer was positioned over the greater trochanter of the femur with the fixed arm in line with the axillary midline of the trunk and the movable arm parallel to the side of the individual's leg over the lateral femoral condyle. The evaluator conducted the limb that was being assessed to the point of mild discomfort, performing hip flexion. Three attempts were made for each limb.4
Strength assessment (isokinetic test)Bilateral isokinetic torque of the knee flexors and extensors was measured using a REV 9000 isokinetic dynamometer (Technogym, Italy). The players were tested in the sitting position, with a 100° angle of the hip. Straps were used to hold the pelvis and trunk in place. The axis of rotation of the dynamometer was aligned with the axis of rotation of the knee (lateral femoral epicondyle). Participants were instructed to keep their hands at the side of the seat during all testing efforts. The range of motion for the test was 80° and 10–90° of knee flexion was used.
The warm-up consisted of two muscle actions at 50% of perceived maximum effort. Next, the individual rested for two minutes and performed five repetitions of maximum intensity of the same muscle action and speed of the warm-up. First the DL was evaluated, and after the NDL. Four warm-up and maximum test sequences were performed: concentric action at 60°s, eccentric at 60°s, concentric at 180°s, and eccentric at 180°s. All sequences complied the same warm-up and test protocol.15
Normative values were considered for the conventional ratio of 60°s between 50% and 70%,16–18 for the conventional ratio of 180°s between 70% and 90%,19 for the functional ratio at 60°s and 180°s between 90% and 110%16,17,20 and for the Q/Q and H/H deficits larger that 15%.17,21–23
Statistical analysisData were analyzed using GraphPad Prism 6.0 software. Initially, the Shapiro–Wilk normality test was performed. To compare the differences between DL and NDL, an independent t-test was used, adopting a level of significance of p<0.05.
ResultsTable 2 presents the results for the evaluation of flexibility in DL and NDL for goniometry.
In relation to the deficit between the DL and the NDL, assuming as normative standard that this value is between −10% and 10%, we found 17% of the young athletes were outside this standard. The same percentage (17%) can be seen for individuals who presented an angle of less than 90° in the evaluation (Table 3).
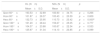
Table 4 shows the results found in the isokinetic evaluation in relation to the absolute PT in the concentric action of the quadriceps and hamstrings and also in the eccentric action of the hamstrings for DL and NDL at angular velocities of 60°s and 180°s. A significant difference was found for the hamstrings in the eccentric action for the 60°s velocity between DL and NDL (p<0.05), indicating a DL significantly stronger than NDL.
Absolute peak torque of the quadriceps and hamstrings of the dominant leg (DL) and non-dominant leg (NDL) at speeds of 60°s and 180°s.
| DL (Nm) | NDL (Nm) | p | |
|---|---|---|---|
| Mean±S.D. | Mean±S.D. | ||
| Qcon 60°s | 193.53±32.89 | 183.90±34.75 | p=0.266 |
| Hcon 60°s | 101.87±26.37 | 100.43±20.59 | p=0.809 |
| Hecc 60°s | 132.73±25.95 | 110.73±23.42 | p=0.000a |
| Qcon 180°s | 161.20±28.44 | 159.27±25.05 | p=0.777 |
| Hcon 180°s | 104.37±23.88 | 100.67±22.34 | p=0.533 |
| Hecc 180°s | 125.97±31.34 | 114.13±23.85 | p=0.099 |
Abbreviations: Q, quadriceps; H, hamstrings; Con, concentric; Ecc, eccentric; Nm, Newton-meter.
Regarding the conventional and functional ratio of DL and NDL at velocities of 60°s and 180°s, a significant difference was observed for the functional ratio at 60°s between DL and NDL (p<0.05) indicating a significantly more balanced DL than the NDL. The values found for the conventional ratio at 60°s and for the functional ratio at 180°/s are close to the normative values, while for the functional ratio at 60°/s and for the conventional ratio at 180°/s the values are below the normative standards (Table 5).
Conventional and functional ratio of dominant leg (DL) and non-dominant leg (NDL) at speeds of 60°s and 180°s.
| DL (%) | NDL (%) | p | |
|---|---|---|---|
| Mean±S.D. | Mean±S.D. | ||
| H/Q con 60°s | 52.94±11.38 | 55.19±9.38 | p=0.397 |
| H/Q fun 60°s | 69.26±12.34 | 61.13±11.41 | p=0.009a |
| H/Q con 180°s | 65.00±10.98 | 63.58±12.62 | p=0.638 |
| H/Q fun 180°s | 79.00±18.49 | 72.94±17.11 | p=0.185 |
Abbreviations: H/Q con, hamstring/quadriceps conventional ratio (concentric hamstring/concentric quadriceps); H/Q fun, hamstrings/quadriceps functional ratio (eccentric hamstring/concentric quadriceps).
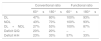
Table 6 shows the percentage quantification of young athletes that were not within the normative standard in the isokinetic test for the conventional ratio and for the functional ratio in 60°s and 180°s in DL, NDL, and both legs (DL+NDL). Besides the deficit between the DL and NDL quadriceps for the concentric action and between the hamstrings of the DL and the NDL for concentric and eccentric actions, at 60°s and 180°s.
Quantity in percentage (%) of the athletes that were not within the normative standard in the isokinetic test.
| Conventional ratio | Functional ratio | |||
|---|---|---|---|---|
| 60°s | 180°s | 60°s | 180°s | |
| DL | 47% | 80% | 100% | 93% |
| NDL | 43% | 70% | 100% | 93% |
| DL+NDL | 27% | 53% | 100% | 87% |
| Deficit Q/Q | 20% | 20% | – | – |
| Deficit H/H | 23% | 33% | 57% | 33% |
Abbreviations: DL, dominant leg; NDL, non-dominant leg; Deficit Q/Q, difference between DL and NDL quadriceps; Deficit H/H, difference between hamstrings of DL and NDL.
The aim of the present study was to compare force levels through isokinetic tests at velocities of 60°s and 180°s, which were observed values of the PT in the concentric and eccentric actions, the conventional and functional H/Q ratio, and flexibility, through goniometry, between DL and NDL of young soccer athletes. The results showed the athletes had an eccentric hamstring action in the DL stronger than in the NDL, besides the DL had a more balanced H/Q ratio than the NDL, indicating strength asymmetry between the limbs and in the same limb.
On the strength, it was possible to observe that the young soccer athletes presented an eccentric action of the DL hamstrings significantly stronger than in the NDL at 60°s, which ended up influencing the H/Q ratio for the functional ratio, where DL was more balanced than NDL, suggesting an asymmetry of limb strength and muscle imbalance. In the study by Bonetti et al.8 investigating also young players, the authors reported the posterior thigh of the DL was significantly stronger than the NDL, besides the DL had a more balanced H/Q ratio than the NDL, at the speed of 60°s. However, the authors only tested the concentric action of both the quadriceps and the hamstrings, using the conventional ratio as a way to evaluate the H/Q ratio. Although we found a stronger DL for the hamstrings and with a lower imbalance compared to NDL, we did not observe this result for the concentric muscular action and for the conventional ratio in 60°s.
It was possible to observe more than half of the athletes (57%) with a H/H deficit in eccentric action greater than 15%. Fousekis et al.,7 in a prospective study, reported soccer athletes who presented an asymmetric eccentric strength in the hamstrings were more likely to have a muscle injury in this region. This event can be explained by the fact the asymmetry in the force of the hamstrings in the eccentric phase causes a decrease in the responsiveness of this muscle to the force created by the quadriceps during a race, for example, which impairs the deceleration phase and can trigger an injury. However, in this study there is no definition of which member had higher levels of strength, because it divided the limbs into right and left, and not into DL and NDL.
Regarding PT for concentric action and conventional ratio at 60°s, and from PT for concentric and eccentric action, and conventional and functional ratio at 180°s, no significant differences were found between DL and NDL. These results are in agreement with those reported by Danejshoo et al.2 for the velocity of 60°s and 180°s in the PT of the concentric action and for the conventional ratio, Śliwowski et al.12 for the velocity of 60°s in the PT of concentric action and the conventional ratio, and by Silva et al.5 for the velocity of 180°s in concentric and eccentric PT, and functional and conventional ratio. What suggests a smaller predisposition of young athletes to possess asymmetries between the limbs for concentric action of the quadriceps and concentric of the hamstrings.
In addition, the majority of athletes presented values for the functional ratio at 60°s and 180°s, and for the conventional ratio at 180°s, at the DL and in the NDL, outside the normative standards. This indicates a lesser action, or an inefficient, eccentric and concentric action of the hamstrings when compared to the concentric action of the quadriceps. Our findings are in agreement with the study by Fousekis et al.,7 which evaluated professional soccer players in the isokinetic at 60°s and 180°s for concentric and eccentric action and 300°s for concentric action, reporting 89% of the sample with at least one isokinetic force variable outside the normative standards. This suggests a greater chance of finding individuals with muscle imbalances in the same limb. Thus, in relation to strength, it is possible to verify that there is still no consensus on the fact whether soccer-specific training influences or not the concentric and/or eccentric strength of the anterior and posterior thighs, whether in comparison to the H/Q ratio or between DL and NDL, in young soccer players.8 This may have occurred due to the non-standardization of isokinetic force evaluation, where studies present different isokinetic evaluation protocols, which may influence the results and also affect when they are compared.
Regarding flexibility, the results of the present study did not show a significant difference between DL and NDL. Most of the athletes (83%) did not present a significant deficit between the limbs and also did not present an angle smaller than 90°. This result is in agreement with studies by Rahnama et al.4 and Bradley and Portas,24 who reported professional soccer players did not exhibit significant differences between limbs. While Daneshjoo et al.2 tested young players and found different results, observing a significantly more flexible DL than the NDL. These divergent results can be explained by the influence on the flexibility from age, training time, type of training, maturational process, and previous injuries, among other factors.
Most studies relating flexibility and soccer choose to use the sit-and-reach test proposed by Wells and Dillon.25 This test assesses the lower limbs bilaterally and it is not possible to compare DL and NDL. Accordingly, there is a need for more studies using goniometry, since it is more reliable and valid to measure posterior thigh flexibility than the sit-and-reach test.26 It is possible to observe that the scientific literature still presents disagreements about the relationship between flexibility and specific soccer training, where the preference for the use of one of the limbs may or may not influence the level of flexibility. In addition to its possible impact on both performance and as a potential triggering factor for injury.27
Regarding the interaction between strength and flexibility, no results were found that could establish a relationship between these characteristics. Daneshjoo et al.,2 analyzing these two characteristics in young soccer players, reported the DL to be significantly more flexible than the NDL and no significant differences in strength, whereas in our study we did not find significant differences on flexibility, but we for relative strength. This conflicting result for strength can be explained by the evaluation of concentric action only, since with this type of contraction we also did not find a significant difference between the limbs. From this, Daneshjoo et al.2 also did not establish any possible interaction between these measurements. However, Fousekis et al.7 evaluating strength and flexibility in soccer players, suggested occurrence of the association of asymmetries of these attributes may potentiate the mechanisms generating muscle injuries. It is noteworthy only Daneshjoo et al.2 examined young soccer players, such that the literature still lacks new studies on the subject, since the results diverge when compared to our study.
In conclusion, soccer-specific training may negatively influence hamstrings muscle strength when comparing DL and NDL, and the balance ratio between the concentric action of the quadriceps and eccentric hamstrings in young soccer players. It is noteworthy that this observation is specific to this sample group, being able to view or not, to other groups of young athletes. Accordingly, it is necessary to evaluate and to plan for training strategies that minimize this imbalance, in order to prevent muscular injuries and provide professional soccer players more adequate training.
Conflict of interestsAuthors declare that they don’t have any conflict of interests.
Club de Regatas Vasco Gama for lending its space and equipment.

