




Sleep is important for athletes to recover from training and competition. However, there are no systematic reports on sleep patterns of elite soccer adult athletes. This article described the sleep pattern of elite soccer athletes and identified it is factors associated. We included only original articles, written in English, and with professional male soccer players aged over 18 years old competing in the first national division. On days without match and at a matchday, the mean of total sleep time, sleep onset latency, and sleep efficiency were less than the National Sleep Foundation's recommendation in almost all articles. Both local and match outcomes can affect the sleep pattern. So, elite soccer athletes are often unable to achieve sleep recommendations. Home matches, defeat, or a draw, as well as travels, are factors that negatively affect the quality and quantity of sleep of the athletes.
Sleep is associated with several physiological processes that aid recovery and adjustments resulting from training and sports competition. During sleep, there is a peak of pulsatile growth hormone release, reduced cortisol release, consolidation of memories, and potentiation of immune responses.1 When sleep deprivation or restriction occurs, the physiological processes can be disrupted, leading to a low ability to recover and adjust to training.2 By contrast, sleep in ideal quantity and quality can favor physical performance,3 and sleep extension can improve sports performance.4 However, this last premise should be viewed with caution.5
Sleep patterns is a personal schedule of bedtime and wake up time.6 With this information, it is possible to describe some variables of sleep, like sleep duration, sleep onset latency (SOL), and sleep efficiency (SE). The recommendations of the National Sleep Foundation (NSF) for adults to get a good quantity and quality sleep is sleep duration > 420 min (min.), SOL < 30 min., and SE > 85%,7,8 and it is considered that athletes may need more sleep duration than most people.9 Regardless of the modality, gender, or sport type (individual vs. team sports), athletes have difficulty getting a good night's sleep, and even elite athletes may have poor sleep quality.10,11 Some of the main factors that negatively alter sleep are the time that competition and training session starts. The competition started after 20h00 and training started until 07h00 have a deleterious effect on sleep.12 Several matches start at 20h45 for the UEFA Champions League, at 22h00 for LALIGA and the First Division of the Brazilian league. At this time, the psychomotor vigilance is lower and there is a greater propensity for sleep onset, however, the athletes are subjected to competitive stimuli that delay sleep onset.13 Considering the match schedule and post-match commitments, athletes can show regular behaviors that will lead to a reduction in the quantity and quality of sleep, establishing a chronic sleep restriction.14
In recent years, the number of publications on soccer athlete sleep has increased.15,16 However, many studies investigated amateur,17 youth,18 or college athletes.19 It is noteworthy that elite athletes train more days and hours, with a greater perceived exertion compared to amateur or semi-professional athletes. These differences may be due to the organization, economic situation, and higher salaries of professional athletes, leading to exclusive dedication.20 College students often report sleep problems,21 and when college students are athletes, they have worse sleep habits than non-athlete college students,22 poor sleep quality and insufficient sleep.23 Thus, the analysis of the sleep pattern of elite soccer athletes is less known in the literature. This review aimed to describe the sleep pattern of elite soccer athletes and identify it is factors associated.
Materials and methodsThis review was conducted following the guidelines of Preferred Reporting Items for Systematic Reviews and Meta-Analyses - PRISMA -24 (Table 1). Two researchers selected articles published in the Cochrane Library, PubMed, Scopus, Web of Science, and SPORTDiscus databases in searches performed in March 2021 and updated in June 2021. The search terms were ("soccer" OR "football") AND (sleep OR "sleep parameters" OR "sleep extension" OR "sleep restriction" OR "sleep deprivation" OR "sleep quality" OR "sleep index" OR "sleep amount" OR "sleep quantity" OR "sleep duration").
PRISMA checklist.
The inclusion criteria were original articles, articles written in English and published in peer-reviewed journals, only professional male soccer players with a mean age over 18 years old and playing in the first national division; and the existence of objective or subjective sleep variables. We excluded articles with athletes undergoing injury treatment, review articles, articles in press, short-communication, and editorials.
Information related to the sample, study design, intervention, and results were extracted from each article. Data reported information on participants (age, nationality), type of analysis (descriptive, experimental, duration of observation, the inclusion of matches), and sleep variables. Sleep variables were obtained from the numerical information of each article. Due to the wide variation in study designs, different variables analyzed, and different instruments used, we did not perform a meta-analysis. Regarding the description of the days before the matchday, the following D- was used, the matchday was defined as D0, and the days after the match were defined as D+.
For the global description of SE, SOL, and total sleep time (TST), all conditions described in the studies were grouped. Two conditions were established for the description of sleep variables: a day with match and days without match. On the matchday, all match conditions described in the studies were grouped. On days without a match, all conditions without a match were grouped, such as training days, travel, or days off.
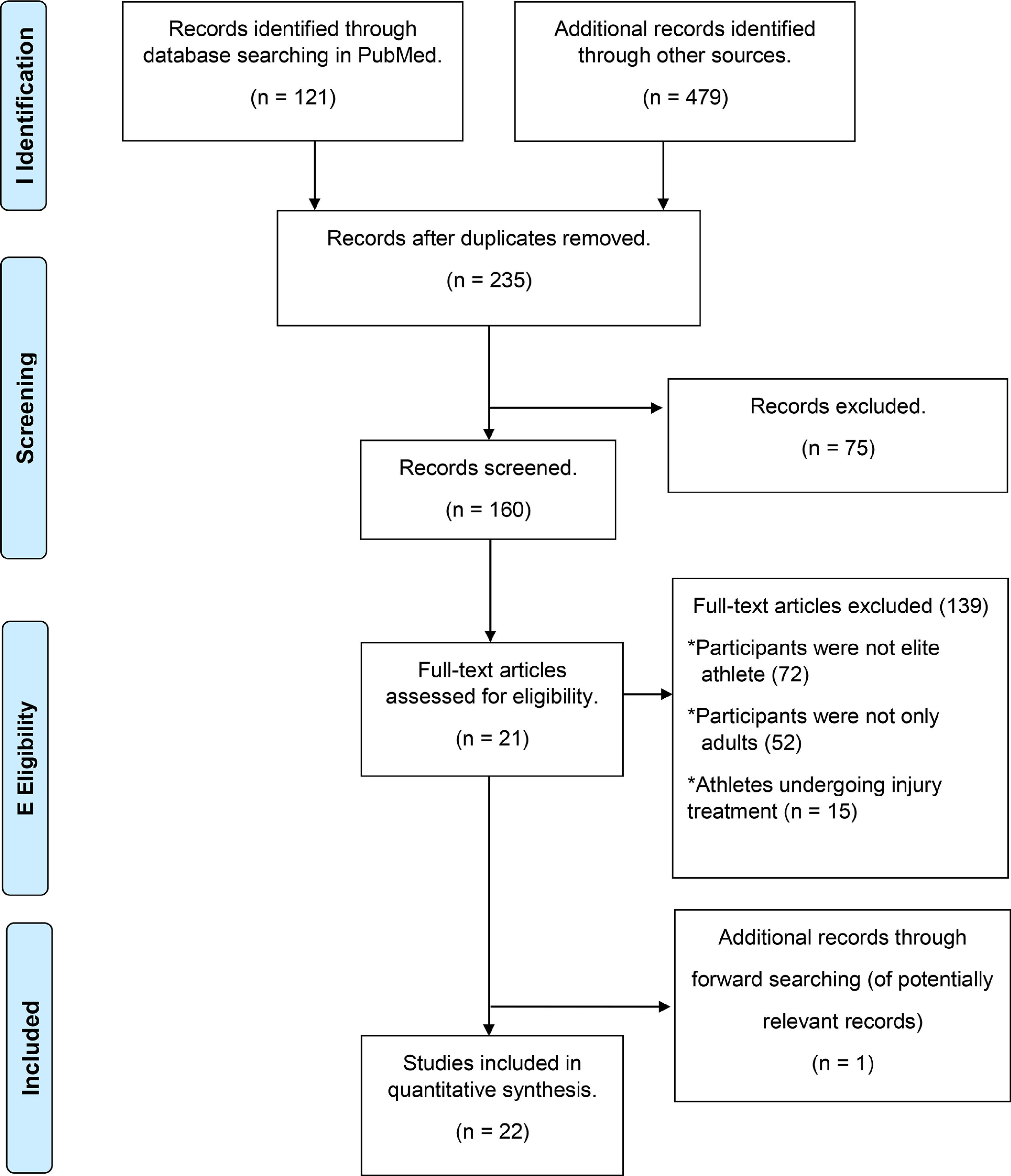
ResultsDetails of the search process are available in Fig. 1. The systematic search found 600 articles. Of these, 121 were found on PubMed, 142 on SPORTDiscus, 161 on Web of Science, and 176 on Scopus. After deleting the duplicate articles, 235 articles remained. Afterward, we excluded 75 articles after reading the titles and abstracts due to not meeting the eligibility criteria. We excluded 138 articles after a complete reading. Thus, we included a total of 22 articles for final review.
All articles were published from 2014 onwards (Table 2). The overall sample was 482 athletes and comprised between one 25 and 111 athletes 26 per study, and the lowest and the maximum mean age was 19.1 27,28 and 31 years old,25 respectively. The studies were carried out in nine different countries, and the country with the highest number of publications was England.27–31 The number of matches per study varied between one32 and 154 matches.15 The number of days before the D0 varied between one30 and nine days,31 and the number of days after the D0 varied between two25,33 and eight days.27,28
General characteristics of the studies.
| Study | Sample | Country | Season | Number of matches per study | |||
|---|---|---|---|---|---|---|---|
| Age (years old) | |||||||
| n | M | ± | SD | ||||
| Fowler et al.33 | 6 | 23.4 | (19.9–25.9)* | Australia | Competition | 12 | |
| Fowler et al.32 | 16 | 27 | (25–29)* | Australia | Competition | 1 | |
| Laux et al.16 | 22 | 25.8 | ± | 5 | Germany | Competition | 74 |
| Thorpe et al.27 | 10 | 19.1 | ± | 0.6 | England | Competition | 2 |
| Buccheit et al.37 | 12 | 24.4 | ± | 5.3 | France | Pre-season | 2 |
| Fullagar et al.31 | 15 | 25.5 | ± | 4.9 | England | Competition | 2 |
| Fullagar et al.34 | 16 | 25.9 | ± | 7.5 | Germany / Netherlands | Competition | 48 |
| Rijken et al.57 | 11 | 22# | 21-32# | Netherlands | - | ND | |
| Thorpe et al.30 | 29 | 27 | ± | 5.1 | England | Competition | ND |
| Clemente et al.38 | 35 | 25.7 | ± | 5 | Portugal | Competition | 53 |
| Fowler et al.36 | 23 | 26 | ± | 4 | Australia | Competition | ND |
| Thorpe et al.28 | 10 | 19.1 | ± | 0.6 | England | Competition | 2 |
| Carriço et al.15 | 25 | 26.3 | ± | 4.7 | Portugal | Competition | 154 |
| Fessi et al.40 | 12 | 25.6 | ± | 3.6 | Qatar | Competition | 52 |
| De Beéck 39 | 26 | 23.2 | ± | 3.7 | Netherlands | Pre-season / Competition | ND |
| Jaspers et al.41 | 26 | 23.2 | ± | 3.7 | Netherlands | Pre-season / Competition | ND |
| Khalladi et al.26 | 111 | 23.7 | ± | 4.8 | Qatar | - | ND |
| Nédélec et al.14 | 20 | 26 | ± | 4.6 | France | Competition | 7 |
| Nédélec et al.25 | 1 | 31 | France | Pre-competition / Competition | 2 | ||
| Silva et al.35 | 23 | 26.5 | ± | 5.2 | Brazil | Pre-season / Competition | ND |
| Selmi et al.42 | 15 | 24 | ± | 1 | Tunisia | Pre-season | ND |
| Springham et al.29 | 18 | 24 | ± | 3.8 | England | Pre-season / Competition | 48 |
*= 95% confidence interval; #=median; ND= not described
The duration of the sleep monitoring varied between six days30 and 16 months16 (Table 3). Sixteen sleep variables were identified, with TST, SE, and SOL being the most used. The awakening's number,15,31,33-35 the bedtime,14,15,31,34,36 the wake up,14,15,31,34,36 and the time in bed also were reported.14,15,25,36 In objective monitoring, the instrument used was actigraphy. Among the seven studies with actigraphy, only two described the minimum movement score (threshold) for characterization of sleep/wakefulness, the intervals (epochs), and the frequency,14,25 and one described the sleep/wake threshold and the interval.35 In subjective monitoring, the well-being questionnaire 27,28,30,32,37-42 and the sleep diary 14,25,32,35,36 were the most used.
Description of the methods and main results of the studies.
| Study | Methods | Main results | |
|---|---|---|---|
| Instruments | Sleep variables | ||
| Fowler et al.33 |
| Variance from mean bedtimeSOLSleep durationWake episodesSEMean wake duration | Greater SOL in away matches.SOL greater in D+1 away match than in D+1 at homeSleep duration and higher number of awakenings in D+2 at home than in D+2 away match.Reduced sleep duration on matchday when compared to D-1 and D+1 for away matches. |
| Fowler et al.32 |
| Sleep durationSleep quality | Shorter sleep duration the night before the travel and at D0 compared to other nights. |
| Laux et al.16 |
| Satisfying the person's sleep | A positive association between sleep quality and increased risk of injury. |
| Thorpe et al.27 |
| Sleep quality | There was no association between training load and sleep quality. |
| Buccheit et al.37 |
| Sleep quality | A reduced sleep quality on the 6th day of camp. |
| Fullagar et al.31 |
| Sleep durationMean bedtimeMean waketimeSOLSEWake episodesWake episodes duration | Shorter sleep duration on travel night compared to Post 1.Lower SE during travel night compared to Post 1 and Post 2.D0 had a shorter sleep duration compared to D+2, D+3, D+4, D+7, D+8, and D+9. |
| Fullagar et al.34 |
| BedtimeAwakening timeSleep onset latencySleep durationWake episodesTotal wake episode durationSleep restfulnessAverage duration of naps | Shorter sleep duration for days with night matches compared to training days and day matches.Less restorative sleep after night matches when compared to training days and day matches. |
| Rijken et al.57 |
| Sleep quality | There was no effect of the intervention on sleep quality. |
| Thorpe et al.30 |
| Sleep quality | Sleep quality was worse on a post-match compared to the pre-matchday.Sleep quality increased from D+1 to D+3. |
| Clemente et al.38 |
| Sleep quality | There was no difference in sleep when one or two matches per week. |
| Fowler et al.36 |
| BedtimeSOLSEWaketimeGet-up timeTIBSleep duration | Shorter sleep duration during the travel when compared to other days.Sleep duration and time in bed reduced on the arrival day when compared to Post 1, Post 2, Post 3, and Post 4. |
| Thorpe et al.28 |
| Sleep quality | There was no association between distance covered at high-speed running and sleep quality. |
| Carriço et al.15 |
| BedtimeAwakening timeTIBTSTSOLSETotal wake episode duration | Lower TST after night matches when compared to training days and day matches.Higher TST in away matches compared to home matches. |
| Fessi and Moalla 40 |
| Sleep quality | Sleep quality was higher in D0 with victory, compared to D0 with defeat or draw.Sleep quality was higher in D0 with a draw when compared to D0 with defeat. |
| De Beéck et al.39 |
| Sleep quality | Sleep had a trivial effect to predict performance. |
| Jaspers et al.41 |
| Sleep quality | The training load did not affect sleep. |
| Khalladi et al.26 |
| Sleep quality | The prevalence of poor sleep quality was 68.5%. |
| Nédélec et al.14 |
| BedtimeAwakening timeTIBSOLTSTSESleep qualitySSQ | Most players (90%) indicated worse sleep quality in the nights after evening matches compared to training days.Bedtime and TST were lower in D0 when compared to training days. |
| Nédélec et al.25 |
| TIBSOLTSTSESSQ | SOL and SE the night before the injury were out of intra-individual variability.SOL in the week before the injury was greater than at baseline.SOL greater at D0 than at baseline.SE was out of intra-individual variability in D0.SSQ was lower in DO than baseline. |
| Selmi et al.42 |
| Sleep quality | Sleep quality increased during the intense training period. |
| Silva et al.35 |
| Sleep durationSESOLTime awake | A moderate negative relationship between SE and injury characteristics.44% of the variance in the number of injuries can be explained by SE. |
| Springham et al.29 |
| Sleep quality | Sleep quality decreased to below baseline values in the first half of the season.Salivary testosterone had a quadratic relationship with sleep quality.Salivary cortisol had a linear relationship with sleep quality.Salivary testosterone: Cortisol had a linear relationship with sleep quality. |
Legend: PSQI, Pittsburgh Sleep Questionnaire Index; SE, sleep efficiency; SOL, sleep onset latency; SSQ, subjective sleep quality; TIB, time in bed; TST, total sleep time.
Overall, the mean TST was less than 420 min. in 58% (23/40) of the conditions. The lowest and highest reported mean TST was 223 31 and 524 min. 34, respectively. The SOL was greater than 30 min. in 46% (18/39) of the conditions. The lowest and highest described mean SOL was 15.8 31 and 159 min. 25, respectively. The SE was less than 85% in 72% (26/36) of the conditions. The lowest and highest reported SE was 68.4% 31 and 93.1%,35 respectively.
In days without a match, the mean TST was less than 420 min. in 43% (12/28) of the conditions, the mean SOL was greater than 30 min. in 43% (12/28) of the conditions, and the mean SE was less than 85% in 63% (17/27) of the conditions. In D0 (Table 4), the mean TST was less than 420 min. in 91% (10/11) of the conditions, the mean SOL was greater than 30 min. in 55% (6/11) of the conditions, and the mean SE was less than 85% in 100% (9/9) of the conditions.
Sleep pattern in matchdays (DO).
| Study | Sleep pattern | Kick-off | ||
|---|---|---|---|---|
| TST (minutes) | SE (%) | SOL(minutes) | ||
| Carriço et al.15 | 349 ± 43 | 79 ± 6 | 32 ± 17 | The kick-off was not described. |
| 333 ± 53 | 78 ± 7 | 35 ± 28 | The kick-off was not described. | |
| 369 ± 60 | 80 ± 8 | 26 ± 20 | The kick-off was not described. | |
| 399 ± 92 | 81 ± 8 | 41 ± 42 | Matches which kick-off before 18h00. | |
| 328 ± 88 | 78 ± 8 | 31 ± 21 | Matches which kick-off after 18h00. | |
| Fullagar et al.34 | 500 ± 41 | – | 22 ± 13 | Matches which concluded before 18h00. |
| 343 ± 96 | – | 26 ± 15 | Matches which kicked off after 18h00. | |
| Nedelec et al.14 | 291 ± 72 | 75 ± 13 | 45 ± 38 | 2 matches at 20h30, one match at 19h00, 2 matches at 18h00. |
| Nédélec et al.25 | 302 ± 77 | 70 ± 10 | 65 ± 35 | Matches which kick-off time between 19h00 and 21h05. |
In D-1, the mean TST ranged from 29432 and 486 min. 31, the mean SE ranged between 81.2 and 86.8%,31 and the mean SOL ranged from 20.6 and 22.5 min. 31. In D0, the mean TST varied between 27231 and 500 min.34, the mean SE varied between 70%25 and 81%,15 and the mean SOL varied between 15.831 and 65 min.25 On D0, one article showed greater total sleep duration in away match compared to home match,15 while other article observed no difference in any sleep parameter for matches played at home or away from home.33 Another point is than on D0, the perceived sleep quality was worst in losing compared to drawing and winning.40 In D+1, the mean TST varied between 343 and 348 min. 31, the mean SE varied between 75% and 77%,31 and the mean SOL varied between 20.9 and 28.6 min.31 When analyzing the training days, the mean TST ranged between 38314 and 537 min. 31, the mean SE ranged between 79.1%14 and 85.4%,31 and the mean SOL ranged between 1634 and 38 min.14
DiscussionThis study aimed to describe the sleep pattern of elite soccer athletes and identify factors that can affect sleep. In general, most athletes do not reach the NSF's recommendation for the adult, a fact that can be aggravated on D0, where 91% of the observed results described the sleep duration below of sleep duration's recommendation. In addition, other factors can affect soccer players' sleep, such as the match location, match outcome, and travel.
In general, the sleep variables monitored in D-1 met the NSF's recommendations.7,8 The schedule of D-1 was different between the studies. In one article the athletes had rest,32 in an article the athletes trained in D-1 and rested in the D-1 of the other match31 and an article did not describe what was done the day before the matchday.33 Interestingly, even with a training session on the day before the D0, the athletes reached the sleep duration recommended by the NSF. Recently, Roberts et al12 found no effect of the night before the sporting event on sleep variables.
Regarding D0, almost all studies indicated that the soccer athlete does not reach the NSF's recommendation. The mean sleep duration of 500 min. was observed when the match was completed until 18h00.32 When the match kicked-off after 18h00, the mean sleep duration was reduced to 343 min. Thus, the end time of the match must be considered when analyzing the athlete's sleep duration on D0. These results can be explained by the match time, which generally delays the SOL, exessive light, intense exercise that increase the core temperature, tension, and arousal of the central nervous system that results from the competition and cheering.14,34 Furthermore, Nédélec et al14 demonstrated that 90% of the players had worse sleep quality in the post-night matches compared to training days, while bedtime and TST were lower post-night matches when compared to training days. The arousal induced by the match, environmental conditions, and behaviors before and after a night match, with naps, caffeine, and alcohol consumption being able to explain the lack of sleep after night matches when compared to training days.10,43
The exact time that the match continues to affect sleep has different results. A match can negatively affect sleep variables at D0 and not show significant differences between D0 and D+1.31,32,34 Differently, sleep quality may take four days to reestablish D-1 values.30 This deleterious effect on sleep patterns may lead to a reduction in a training capacity and a consequent reduction in high-level match actions. Depending on the schedule in which the team is inserted, the athlete will have negatively altered sleep and, consequently, will increase the risk of injury and reduce their capacity for high performance.
Few studies described the minimum duration that the athlete should play to be included in the analyses.30,31,34,40 The absence of this information in 80% of the studies must be considered when interpreting the results. The physical and technical performance can be different if the athlete was a starter or a non-starter.44,45 If the athlete was substituted in the first half, the residual effect of the match could be smaller than those who participated in the full match. The same can be considered for athletes who were substituted in halftime or athletes who entered the final moments of the match. So, it will be hard to understand if what affected the sleep pattern were the physical demands and their residual effect or were the professional and personal commitments that occur after the match. Therefore, further studies must describe the time the athlete was present at the match and, if possible, the external load that he was submitted.
The match location affected some sleep variables, such as higher TST and SE at D0 in away matches. It is suggested that social commitments have a greater influence in home matches, considering that there is no need for return travel, thus, athletes can spend more time with friends or family. Fowler et al33 found no statistically significant difference in sleep variables when comparing home and away matches in D0. However, they observed in home matches, large effect size indicating lower SOL in D-2, lower bedtime variance in D-1, lower TST in D+1, and higher TST and number of awakenings in D+2. The authors argue that the fact that coaches and staff stayed with the players in the hotel facilitates the monitoring of the athletes' sleep.
However, some aspects should be considered. Home teams have an advantage in winning the disputed points.46 Consequently, the match outcome may have impacted the sleep pattern.40 Besides, the distance from away matches and the time spent to the place where the night's sleep would be monitored. In some countries with a smaller geographic area, away matches may take place over shorter distances than in countries with larger areas. Thus, it is essential to describe the time spent going to bed to understand the real effect of localization. In addition, there are leagues in which teams from the same local duel each other (e.g., Flamengo x Fluminense, both teams from Rio de Janeiro and participate of First Division of Brazilian league), thus, the home factor becomes irrelevant, considering that the sleeping location will not be affected. Consequently, more information should be provided by articles describing the effect of match location on sleep variables.
Sleep quality was worse when the match outcome is defeat, compared to winning. Besides, the sleep quality on nights with a draw was worse when compared to winning. In the post-match with defeats, the worsening in sleep quality is accompanied by an increase in perceived stress and fatigue, which can be explained by the reduction in post-match testosterone with defeat.40 Studies corroborate this information, showing that perceived stress is positively associated with worsening sleep quality47 and the reduction in perceived stress predicts the improvement in sleep quality.48 Evidence indicates that stress can trigger an increase in anxiety, which can lead to physical activation, nervousness, and apprehension, and consequently, affect sleep quality.49-51 Fessi and Moalla40 did not describe the bedtime or wake up, which may omit an acute sleep restriction, and consequently affect the sleep quality. Another feature not described is whether the match was played away or at home, even if defeat or draw in away matches is more common.46 As described above, the match location can negatively affect the sleep variables. Thus, current information on the effect of the match outcome on sleep is still scarce and more studies are needed.
Results regarding the impact of the training session on sleep variables were contradictory. Two studies showed that athletes achieve sleep recommendations.31,34 Both studies did not describe the times that the training sessions started. Even with athletes being recommended to stay at least 10 hours in bed, Nédélec et al14 identified that they did not reach the NSF's recommendation. Interestingly, despite the start of training sessions after 10h00. This inability to achieve the proper sleep duration may be due to the use of social media, cell phones, games, computers, television, competition anxiety, or performance concerns.10,52
Training load (TL) does not seem to affect the athlete's sleep. Three studies found no relationship between TL and sleep.27,28,41 These results are the opposite of those observed in Australian football players, where TL was related to sleep during pre-season.53 When an intense training period occurs in soccer, sleep can be impacted.42 In the studies included in this review, sleep was monitored during the competition phase, and due to the number of matches played, training sessions can be established more to recover the athletes or maintain the level of physical fitness, when they are considered the starting athletes, consequently, less oscillation in the internal TL and external TL would not be enough to relate to the alterations in the sleep pattern.
In the articles described above,27,28,41 both authors did not describe the awakening time and the schedule of the training sessions. If the athlete is sleep-restricted, the performance in the activity may be reduced. A single sleep-restricted night can affect sports performance, especially in specific sport skills.54 In addition, the time the activity is performed interacts with the previous waking period, where the greater the vigil, the greater the deleterious effect of sleep restriction on the observed variable.55 Consequently, if the training session occurs in the afternoon, the reduction in sports performance will be greater. Therefore, there will be an effect of this sleep restriction on performance, causing lower TL. Thus, future studies should describe sleep variables, training schedule, and internal TL and external TL to verify the association between sleep and TL.
Studies relate sleep deprivation with the occurrence of musculoskeletal injuries in athletes, due to reduced levels of testosterone and growth hormone, and increased cortisol, important hormones in the process of protein synthesis and degradation.56 Overall, the studies in this area indicate an association between sleep and injuries. Silva et al,35 assessed sleep during the pre-season, however, injuries included in the study were recorded up to six months after sleep analysis. Thus, sleep was not assessed at the same time as the athlete's injuries. Injuries have multifactorial causes, and in this study, it was not analyzed hormonal and psychological responses, as training and accumulation of disputed matches may have contributed to results. In the study of Laux et al,16 the sleep quality was assessed only by a Likert scale (REST-Q questionnaire), which may provide false reports, underestimating or overestimating results. Although the research lasted 16 months, the subjective sleep assessment was only recorded once every 4 weeks. It was not possible to obtain sleep data always before each match. Nédélec et al25 did not record previous injuries as a risk factor for injuries that occurred during the assessment, which made it impossible to analyze whether the injuries were recurrent.
The night before the travel and the night's travel negatively affected sleep. Fowler et al32 examined the effect of 10-hour travel across 1-time zone on sleep duration. The authors found that sleep duration was shorter the night before the travel when compared to other nights. This result is explained by the fact that players need to wake up at approximately 4h00 to travel. Fullagar et al31 evaluated the sleep on an international flight to the west, totaling 18 hours of travel and 4 time-zones shifts. The sleep duration on night's travel was shorter when compared to the first night of recovery, and the SE was lower during the travel compared to the first and second's recovery nights. The reduced sleep duration and poorer sleep quality during travel can be explained by noise and the air pressure inside the cabin, the timing of the meal, and inadequate sleeping positions. Fowler et al36 investigated the sleep duration during trans-southern travels. On this travel, the delegation took three flights, totaling 19 hours and 11 time zones, and the arrival time at 20h30. They found that the sleep duration was shorter during the travel when compared to the other days. Although athletes travel in business class and can sleep in the supine position, flight connections, and stopovers, the timing of the meal, and cabin lighting can disrupt sleep and shorten sleep duration. Fowler et al32 observed the shortest sleep duration the night before the travel when compared to the other nights. Fullagar et al31 could not obtain objective sleep data from the players before the match, as the athletes were from different countries, so an online subjective sleep survey was used to collect initial measures of this variable. Furthermore, a sleep diary was not used during the travel, which limits the records of information about this period of rest. Fowler et al36 did not record naps, which can be considered a limitation, since the objective of the research was to investigate the sleep duration during long-haul transmeridian travel and that in this type of travel there is usually an increase in the number of naps and sleep night may present worse results since it does not represent the traveler's biological night. Thus, the lack of this data can contribute to reducing the sleep duration found. The sleep variables in this study were obtained only by self-report, which may underestimate or overestimate the results. Buccheit et al37 found a small reduction in sleep quality on the sixth day after travel with six time-zones shifts. Although sleep quality was assessed before, during, and after the travel, the authors used only self-report data. Overall, this information is essential for soccer professionals. Considering that countries like France, Germany, and Brazil are continental countries, teams are constantly traveling and competing, with few days to recovery, which can lead to chronic sleep restriction of athletes.
This study used only adult athletes who were playing in the first division, therefore, extrapolations of athletes from lower divisions and for athletes from the youth category should be viewed with caution. The studies did not describe in their methods whether the analyzes dealt with regular or reserve players, in this sense, it is recommended that future studies describe the percentage of participation of athletes in each match. It is recommended that when evaluating the match outcome, in the case of a cup, whether the evaluated team was successful (classified or disqualified) and in the case of a league, describe the team's position. It also adds up to the fact that the number of sleep nights observed was small, which limits the athlete's sleep pattern throughout the entire season. In addition, the number of players, matches played, and training sessions analyzed were small, possibly not enough to affect the analyzed variables, in addition to statistically influencing the results. The number of subjective instruments used in the studies varied widely, which makes it difficult to compare the sleep variables obtained in each study. Finally, it is important to state that almost all overall the studies included in this review were not experimental studies. At this point, the differences in some sleep patterns should be viewed most as associated or candidate determinants to changes, more than a real cause-effect relationship.
The elite soccer athlete may not reach the sleep recommendation for adult healthy on training days. On matchdays, sleep variables are even worse, and it may take up to four days to return to the pre-values match. The long-term sleep debt of these athletes can lead to reduced sports performance and increase the risk of injury. About travel, attention must be paid to departure and arrival time, so that athletes do not need to wake up early and do not arrive at their destination at a time close to bedtime. In addition, the scheduling of training sessions on the day after the match must be carried out at a time that is possible for all athletes to reach the number of hours and quality of sleep to recover from the previous match. If the match is played at home and the match outcome is defeat, more attention should be paid to the athletes. Thus, the technical committee and the medical department must interact with the athletes to raise awareness and establish strategies that can help the athletes achieve their sleep hours recommendations. As well as evaluating and identifying athletes who present complaints or sleep disorders, so that they can be treated and have a good physical and cognitive recovery during sleep.
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.

