







The prevalence of fibromyalgia in developed countries is over 2.1%. Nowadays, there is no effective treatment for it and different mitigating treatments such as therapeutic exercise are performed instead. In recent years, supplements have also emerged.
ObjectivesTo review and update the evidence on treatment of fibromyalgia symptoms with therapeutic physical exercise and supplements. To achieve this, treatment application times and the duration of treatment programs will be considered.
MethodsA bibliographic search was carried out on Pubmed database. As a result, 695 studies on therapeutic exercise and 53 on supplements were found. From these, 18 therapeutic exercise studies and 8 supplements studies were selected. They were all chosen and assessed according to their methodological quality, which was measured using the PEDro scale.
ResultsEvidence showed that pain and quality of life are improved by the practice of almost any type of physical activity and the intake of Q10 coenzyme or vitamin D supplements. Sleep quality is enhanced by combination of physical exercise and relaxation. Depression, anxiety and mood are improved by the performance of aerobic, flexibility exercises and aquatic biodance.
ConclusionsTherapeutic physical exercise and supplements may be an interesting alternative or complement when treating some fibromyalgia symptoms.
La prevalencia de fibromialgia en los países desarrollados es superior al 2,1%. Actualmente no existe ningún tratamiento eficaz para combatirla y, en su lugar, se efectúan distintos tratamientos para mitigarla, como el ejercicio terapéutico. En los últimos años también han surgido suplementos.
ObjetivoRevisar y actualizar la evidencia sobre el tratamiento de los síntomas de la fibromialgia con el ejercicio físico terapéutico y suplementos. Para lograrlo se revisan los tiempos de aplicación del tratamiento y la duración de estos programas de tratamiento.
MétodosSe realizó una búsqueda bibliográfica en la base de datos PubMed. Como resultado se encontraron 695 trabajos sobre ejercicio terapéutico y 53 sobre suplementos. A partir de estos se seleccionaron 18 estudios de ejercicio terapéutico y 8 de suplementos. Todos ellos fueron seleccionados y evaluados en función de su calidad metodológica, que se midió utilizado la escala PEDro.
ResultadosLa evidencia mostró que el dolor y la calidad de vida mejoraban con la práctica de casi todo tipo de actividad física y con la ingesta de la coenzima Q10 o suplemento de vitamina D. La calidad del sueño mejora mediante la combinación de ejercicio físico y relajación. La depresión, la ansiedad y el estado de ánimo mejoran con la práctica de ejercicio aeróbico, ejercicios de flexibilidad y biodanza acuática.
ConclusionesEl ejercicio físico terapéutico y los suplementos pueden ser una alternativa o complemento interesantes en el tratamiento de algunos síntomas de la fibromialgia.
Fibromyalgia is a syndrome characterized by general and widespread pain as well as depression, digestive disorders, fatigue and sleep disturbance.1 The World Health Organization also includes the presence of other symptoms such as cephalea, irritable bowel, painful menstruation, irritability, thermal sensitivity, fatigability and articular rigidity.2 This disorder is nowadays one of the most serious health issues in our country, as its prevalence rate in develop world countries is 2.1%.3 The American College of Rheumatology states a diagnose using nociceptor sensitization at a 4kg/cm2 pressure of 11 points out of 18 (previously stated) with a development period of at least 3 months.1,4
Several studies have tried to clarify its etiology, which still remains unknown. Some of these argue that there is an alteration at the level of the neuroendocrine system. Here, a hyporeactivity is produced because of hypothalamic–pituitary–adrenal axis fatigue. This affects metabolism, stress levels and immunologic system.5 A prolonged exposure to stress would rend certain glandules unable to produce enough hormones in order to maintain the level of alert. As a result, patients would experience symptoms such as fatigue and muscle pain.5 On the other hand, a recent study shows that pain experienced by fibromyalgia patients may be produced by the vasodilation of hypothalamus-controlled meta-arterioles, as these may cause patient's body temperature deregulation as well as higher lactic acid accumulation in soft tissues.6 Other hypotheses attribute the cause to local alterations, for instance the higher incidence of myofascial trigger points in patients with fibromyalgia.7
No treatment has nowadays proved to be effective when treating fibromyalgia. As a consequence, we focus on the isolated treatment of the different symptoms, mainly using drugs such as analgesics, opioids and antidepressants.8 Nevertheless, pharmacological treatment proves not to be very effective to experience long-term pain relief, diverse side effects may appear and dependency and tolerance risk may arise in patients who have been exposed to a long-term opioid analgesic therapy.8 This obviously shows it is necessary to find innovative therapeutic solutions so as to minimize side effects and improve symptoms.8 Health expenditure levels destined to fibromyalgia raise every year9 and because of this, it is highly advisable to know the possible effects of less expensive new treatments which may prove to be more effective.
Therapeutic exercise is presented as an extraordinarily interesting alternative to fibromyalgia pain treatment in its different approaches.8 There is evidence on its utility to treat the different symptoms of fibromyalgia8 and the number of studies proving this has notably increased in recent years compared to some years ago,10,11 mainly because physical exercise constitutes a safe approach and does not present any side effects. Among the reasons why it may help to attenuate fibromyalgia symptoms, we can also mention that aerobic exercise increases blood irrigation to muscles and as a result, these receive more oxygen and the apparition of trigger points is reduced. Furthermore, doing moderate exercise encourages parasympathetic nervous system activation, which reduces the basal activity of the organism and at the same time favors patient's rest and sleep. Finally, strength training activates both the immune and the endocrine system.12
On the other hand, the increase in the number of studies dealing with the use of supplements to fight with fibromyalgia symptoms has been remarkable in recent years. Several supplements, for instance vitamin D13,14 or coenzyme Q1015–17 seem to produce antioxidant effects, which act at mitochondrial level and on the organism energetic metabolism. This results in an improvement in fatigue, pain and quality of life of fibromyalgia patients.17
The aim of this study is to know the effects and the effectiveness of several therapeutic exercises as well as dietary and pharmacologic supplements to treat pain, quality of life, depression and sleep quality in fibromyalgia patients by revising already published researches on this field. This will enable us to establish some recommendations on therapeutic physical exercise and supplements for patients according to their symptoms.
MethodsA bibliographic search on the kind of exercises performed to fight fibromyalgia symptoms8 was carried out. The available literature on Medline database through Pubmed from November 1, 2010 to November 1, 2015 was reviewed. The inclusion criteria were clinical trials included in studies based on participants suffering from fibromyalgia and published from 2010 in English or in Spanish. The exclusion criteria were articles based on unfinished studies or on researches whose intervention area did not deal with physiotherapy or therapeutic exercise.
The terms employed for this search were “fibromyalgia”, “treatment” and “therapy” combined with the Boolean operator “and” and the term “exercise”. As a result, 695 studies were found. Inclusion criteria were met by 18 of these studies (Fig. 1).

Furthermore, another search was performed in order to know the utility of supplements to treat fibromyalgia symptoms. Again, the source selected was Medline through Pubmed and this time the keywords were “fibromyalgia” and “supplements”, joined by the Boolean operator “and”. There were 53 results and only 8 of these studies met the established inclusion criteria (Fig. 2).

In order to validate the methodological quality of the selected studies, the Physiotherapy Evidence Database (PEDro) scale was used. It presents 11 answer items (“yes”, “no”, “no information”). Only 10 of them were evaluable due to the fact that the first one cannot be counted, as it refers to the external validity of the study. One point is given to “yes” items, whereas no punctuation marks were given to the rest of them. Some authors, for instance Moseley et al.19 state that obtaining 5 punctuation marks or more means a good methodological quality and low risk of bias.18
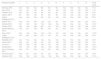
ResultsIn total, 18 studies about physical exercise were analyzed. Those met the established inclusion criteria. According to PEDro scale, there was a good-excellent methodological quality. Punctuation marks ranged from 6 to 10 points out of a maximum of 10. The average value (standard deviation) was 7.83 (1.54) (Table 1). Concerning supplements, 8 studies were analyzed in total. Their methodological quality was good-excellent in 5 of them and poor in 3. Punctuation marks ranged from 4 to 10 and the average value was 7±2.56 (Table 2). Because of the lack of published data on this topic, lower quality studies were also considered.
Results of application of methodological-quality scale PEDro to research studies on PE.
| Research studies | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Final score |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sañudo, 2015 | Yes | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | 7/10 |
| Gavi, 2014 | Yes | No | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 7/10 |
| Gianotti, 2014 | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 6/10 |
| Latorre, 2013 | No | Yes | Yes | No | No | No | Yes | Yes | Yes | Yes | 6/10 |
| López-Rodriguez, 2013 | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8/10 |
| Kaleth, 2013 | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | 8/10 |
| Sañudo 2012 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 10/10 |
| Hooten, 2012 | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8/10 |
| García-Martínez, 2012 | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 6/10 |
| Kayo, 2012 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 10/10 |
| López-Rodriguez, 2012 | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 6/10 |
| Baptista, 2012 | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 9/10 |
| Jones, 2012 | Yes | No | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 7/10 |
| Liu, 2012 | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 9/10 |
| Sañudo 2011 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 10/10 |
| Arcos-Carmona, 2011 | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 8/10 |
| Fontaine, 2010 | Yes | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 6/10 |
| Sañudo, 2010 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 10/10 |
1, random allocation; 2, concealed allocation; 3, initial comparability; 4, blinding of subjects; 5, blinding of therapists; 6, blinding of assessors; 7, appropriate follow-up; 8, intention-to-treat analysis; 9, between-group statistical comparison; 10, point and variability measures; PE, physical exercise.
Results of application of methodological-quality scale PEDro to research studies on supplementation.
| Research studies | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | Final score |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Wepner, 2014 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 10/10 |
| Miyamae, 2013 | No | No | Yes | Yes | No | No | Yes | Yes | Yes | Yes | 6/10 |
| Cordero, 2013 | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes | Yes | 9/10 |
| Alves, 2013 | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | 10/10 |
| Cordero, 2011 | No | No | No | No | No | No | Yes | Yes | Yes | Yes | 4/10 |
| Matthana, 2011 | No | No | Yes | No | No | No | Yes | Yes | Yes | Yes | 5/10 |
| Naziroglu, 2010 | Yes | No | Yes | Yes | No | Yes | Yes | Yes | Yes | Yes | 8/10 |
| Merchant, 2000 | No | No | Yes | No | No | No | Yes | Yes | No | Yes | 4/10 |
1, random allocation; 2, concealed allocation; 3, initial comparability; 4, blinding of subjects; 5, blinding of therapists; 6, blinding of assessors; 7, appropriate follow-up; 8, intention-to-treat analysis; 9, between-group statistical comparison; 10, point and variability measures.
These are the kind of physical exercises to treat fibromyalgia which were extracted from the chosen studies: four studies were based on aerobic exercise,19–22 four studies were based on strength exercises performed with aerobic exercises,23–26 two studies were based on the results of strength exercises compared to those of aerobic exercises or walking,27,28 one comparative study of strength and flexibility exercises,29 one study exclusively based on strength exercises, one study about a half an hour increase in daily activity together with habit reeducation,30 two studies based on aquatic biodance,31,32 one study based on belly dance, one study based on Tai-Chi and finally, one study based on Qigong33 (Table 2). Most of these studies present a duration of 4.38±1.94 months, a range of 3–9 months and a sample of 62.5±36.36 subjects (Table 3).
Characteristics of clinical studies consulted to elaborate the revision on physical exercise.
| Authors, year of publication | Exercise performed | n | Kind of research study | Duration | Results |
|---|---|---|---|---|---|
| Sañudo, 2015 | AER 60–65% MHR | 28 | RCT | 45–60min, 2w, 6 months | Improves DEP and anxiety |
| Kaleth, 2013 | AER 40–65% MHR vs AER+motivation | 170 | RCT | Progressive 10–30min increase, 2–3w, 9 months | Improves pain in group AER+motivation with no differences in group QOF |
| García-Martínez, 2012 | AER 60 at 85% MHR | 26 | RCT | 60min, 3w, 3 months | Improves QOF and MO |
| Arcos-Carmona, 2011 | AER in water and RELAX | 56 | RCT | 30min water and 30min of relaxation, 2w, 2.5 months | Improves QOF, SQ and anxiety |
| Hooten, 2012 | EDU+AER 70% MHR vs EDU+STR | 69 | RCT | 30min/day in 3w | Both improve pain in a similar way |
| Gianotti, 2014 | AER+STR | 32 | RCT | 60min, 2w, 2.5 months | Improves SQ and QOF |
| Sañudo, 2012 | AER 65–70% MHR+STR | 41 | RCT | 45–60min, 2w, 6 months; $=2.5 years | Improves QOF and DEP when compared to initial data. Improvement levels are maintained during follow-up |
| Sañudo 2011 | AER 65–70% MHR+STR | 42 | RCT | 45–60min, 2w, 6 months | Improves QOF |
| Sañudo, 2010 | AER 65–70% MHR VS AER 56–70% MHR+STR | 64 | RCT | 45–60min, 2w, 6 months | Improves MO and QOF in both tre groups with no differences |
| Latorre, 2013 | STR in water and out of water | 72 | No RCT | 60min, 3w, 6 months | Improves MO and QOF |
| Gavi, 2014 | STR vs FLEX | 66 | RCT | 45min, 2w, 4 months | STR improves pain, FLEX improves anxiety, both improve QOF with no differences |
| Kayo, 2012 | Walking vs STR | 90 | RCT | 3w, 4 months, $=3months | Both improve QOF and pain |
| Fontaine, 2010 | 30min increase in daily PA vs EDU | 92 | RCT | 6 sessions of 60min in 3 months | Improves pain and QOF in non-active subjects |
| López-Rodriguez, 2013 | Biodance vs STE | 59 | RCT | 60min, 2w, 3 months | Biodance improves SQ, anxiety, QOF and pain when compared to STE |
| López-Rodriguez, 2012 | Biodance vs STE | 31 | RCT | 60min, 2w, 3 months | Biodance improves pain, QOF and DEP |
| Baptista, 2012 | Belly dance | 75 | RCT | 60min, 2w, 4 months | Improves pain, QOF and MO |
| Jones, 2012 | Tai-chi vs EDU | 98 | RCT | 90min, 2w, 3 months | Tai-chi improves QOF, pain and SQ when compared to a EDU |
| Liu, 2012 | Qigong | 14 | RCT | 15min, 2/day, 6w | Improves pain, QOF and SQ |
STR, strength training; AER, aerobic exercise; FLEX, flexibility exercises; RELAX, relaxation techniques; MHR, maximum heart rate; PA, physical activity; EDU, patient's education; STE, stretching exercises; QOF, quality of life; MO, mood; DEP, depression; SQ, sleep quality; tre, treatment; w, week; $, follow-up after intervention; RCT, randomized clinical trial; No RCT, non-randomized clinical trial.
Concerning the studies based on supplements, two of them dealt with coenzyme Q10,15–17 two studies focused on vitamin D,13,14 one study was based on vitamins C and E joined with exercise performance,34 one study was about creatine35 and finally one study on the Chlorella pyrenoidose algae.36 The duration of all of these studies on supplements was variable. The average duration was 22.14±16.07 weeks. This result shows practically no variation when data are extracted from the two low methodological quality (22.2±17.01 weeks). The average number of participants shows no variation either when the three poor methodological quality studies are excluded (43.4±24.69 participants) compared to 42.5±33.29 participants when all studies are considered (Table 4).
Characteristics of clinical studies consulted to elaborate the revision on supplementation.
| Authors, year of publication | Supplement(s) | n | Kind of research study | Duration | Results |
|---|---|---|---|---|---|
| Wepner, 2014 | Vit D, 20ng/mL | 30 | RCT | 49w | Improves pain; QOF, ANS, DEP do not improve pain |
| Miyamae, 2013 | Co Q10 (Ubiquinol-10) | 77 | No RCT | 28w | Young FBM improves fatigue |
| Cordero, 2013 | Co Q10, 300mg/day | 20 | RCT | 40 days | Improves pain, QOF and fatigue |
| Alves, 2013 | Creatine, 20g/day | 28 | RCT | 16w | It does not improve pain; QOF, DEP only improve strength |
| Cordero, 2011 | Co Q10, 300mg/day | 5 | Cases | 9 months | Improves pain and QOF |
| Matthana, 2011 | Vit D, 50IU/w | 100 | Cohorts | Until Vit D levels reached 50ng/mL | Improves pain and QOF |
| Naziroglu, 2010 | Vit C and E+Exercise | 62 | RCT | 12w | No changes in pain |
| Merchant, 2000 | Chlorella pyrenoidosa, 10g+10mL | 18 | Cohorts | 2 months | Improves pain |
Co Q10, coenzyme Q10; Vit, vitamin; RCT, randomized clinical trial; No RCT, non-randomized clinical trial; w, weeks; QOF, quality of life; ANS, anxiety; DEP, depression; FBM, fibromyalgia.
According to obtained data in our revision session, the kind of supplements and the exercises which could be beneficial for fibromyalgia patients in order to treat their symptoms are diverse. Because of symptom variability in fibromyalgia, the kind of therapeutic exercise and supplements studied have been grouped according to the symptom which proves to be beneficially influenced.
According to Kaleth et al.,21 aerobic training at 40% of maximum heart rate (MHR) in a 10-min period of time and progressively incrementing in nine months until reaching 65% AHR in 30min seems to improve pain, as this does not progress and the initial AHR remains at 40%. In the same line, Fontaine et al.30 suggest that pain improves in fibromyalgia patients who spend at least 30min on mild daily physical activity in a 3-months period of time. These studies seem to show that all kinds of increase in physical activity – even if this increase is minimum – result in remarkable effects on pain relief. This finding may be of special importance in the case of individuals who present high pain or disability levels.
Concerning strength training, Gavi et al.29 and Kayo et al.28 have proven remarkable pain relief. Nevertheless, Hooten et al.,27 have stated no difference in pain relief when following strength training or aerobic exercises programs at 70% AHR. As a result, beneficial effects in pain relief of both training programs have been proved with no difference among them. This finding may prove that aerobic training at 70% AHR as well as strength training may be useful at the same level. This allows us to choose the most appropriate kind of training program for each patient.
Other therapeutic exercise activities, for instance aquatic biodance show a significant quality-of-life improvement when compared to the effects of stretching treatments.31,32 Concerning Tai-chi,37 Qigong33 and belly dance,38 they also seem to have a significant quality-of-life improvement when compared to the effects of habitual patient care. Fontaine et al.,39 have reported a quality-of-life improvement when mildly augmenting the duration of daily physical activity – from 30 to 60min of daily activities performance.39
With regard to supplements, Alves et al.,35 report that a quantity of 20g of creatine per day does not improve quality of life. Wepner et al.13 do not report any improvement neither when administering 20mg/mL of vitamin D. However, Matthana14 argues that the quality of life of patients does improve when administering 50ng/mL of vitamin D. This difference in findings may be due to bias in the study by Matthana, for instance the lack of control and placebo groups or the administration of an insufficient dose by Wepner. As a consequence, vitamin D cannot be recommended in order to improve patients’ quality of life until further reliable data are published. Several studies by Cordero et al.16,17 state that the quality of life of 25 fibromyalgia patients did improve when a dose of 300mg of coenzyme Q10 per day was administered. Similar results were proven by Matthana; nevertheless, in this study vitamin D substituted coenzyme Q10. The quantity administered was 50ng/mL per patient.14
Considering the information extracted from all the studies previously mentioned, it can be stated that any increase in physical activity positively influences quality of life. Strength training and aerobic exercise programs at 45–85% MHR as well as the combination of these or the performance of activities such as aquatic biodance, Tai-chi, Qigong or belly dance improve quality of life in a major extent than education or habitual patient care. Stretching treatments also improve quality of life, although their effect is less important than that experienced when performing strength training or aquatic biodance. In addition, the intake of coenzyme Q10 and vitamin D may also have beneficial effects; however, further studies on the combination of these with other therapies are required.
Therapeutic physical exercise is also remarkably influential when dealing with depression, anxiety and mood. Several studies performed by Sañudo et al. suggest that aerobic exercise performed in 45–60min sessions, 2 days per week in a 6-months period of time significantly improves depression,24,40 anxiety40 and mood.26 García-Martínez et al.22 reach the same conclusion concerning mood and Arcos-Carmona et al. concerning anxiety20 when similar exercising patterns are followed. Sañudo et al. do not find any differences in the benefits of aerobic exercise when strength training programs are added.26 This fact seems to prove that aerobic exercise is more useful than strength training to improve mood. Gavi et al.29 found similar results. In this study, anxiety decreased in a higher extent in patients who participated in flexibility exercises when compared to results obtained with the performance of strength training exercises.
Meanwhile, studies carried out by López-Rodríguez et al.,31,32 show that aquatic biodance improves anxiety32 and depression31 in fibromyalgia patients. Belly dance also improves mood when practiced twice a week during several months.38
No studies which improve mood in fibromyalgia patients using supplements have been found. At the same time, no changes when using vitamin D have been found by Wepner et al.13 The same occurs when a daily supplements of 20g of creatine is administered.35
Sleep quality is a strategic aspect in any patient who suffers from chronic pain. The same happens when fibromyalgia chronic pain is concerned.41 Tang et al. show a relationship between sleep quality and a higher capacity to do physical exercise in fibromyalgia patients.42 As a result, sleep quality is considered as an important aspect concerning treatment.
Arcos-Carmona et al.20 report that performing aerobic exercises in water followed by relaxing exercises in sessions of 60min, twice a week in a period of time of two months and a half significantly improves sleep quality in fibromyalgia patients. A similar result was found by Giannotti et al.,23 who employed the performance of both aerobic and strength exercises in sessions of an hour, twice a week in a period of time of 10 weeks.
Practicing activities such as aquatic biodance32 and Tai-chi37 twice a week in a two months period of time show significant benefits on fibromyalgia patients’ sleep quality.32,37 Liu et al.,33 show very similar results. In this study, a reduced group do Qigong in 15-min sessions, twice a day and during six weeks.33
When considering data included in the studies consulted, it can be concluded that the influence of supplements on sleep quality still remains unknown due to the fact that no study dealing with this topic has been published.
Taking into consideration all the information mentioned above, the following recommendations for treating fibromyalgia symptoms by performing therapeutic physical exercise can be established:
- -
Pain: any physical activity which progressively increases the amount of work and which is regularly practiced in 45–60min sessions, twice or three times a week: strength training, aerobic exercise, aqua exercises, dance activities, Tai-chi, Qigong, walking, etc.
- -
Quality of life: aerobic exercise performed in 60-min sessions, three times a week and activities which require dynamic mobilization of the whole body – for instance, dance activities, Tai-chi or Qigong – twice a week.
- -
Depression, anxiety and mood: regular practice or aerobic and flexibility exercises as well as dance activities in 45–60min sessions, twice a week.
- -
Sleep quality: it is advisable to regularly combine aerobic exercises with relaxation or strength training in 60-min sessions, twice a week. Activities such as aquatic biodance, Tai-chi or Qigong can help when practiced twice a week in sessions of 60min.
It is generally recommended that fibromyalgia patients who present all the symptoms mentioned above do aerobic exercise combined with a progressive-load strength training program in 60-min sessions, three times a week. It is also advisable that they spend two hours per week on dance activities, Tai-chi, Qigong or similar. The intake of 300mg/day of coenzyme Q10 or maintaining more than 50ng/mL of vitamin D levels is also recommended.
The lack of research on supplements to treat fibromyalgia should be mentioned as a limitation of this study. In addition, some information may have been missed due to the fact that only the works on therapeutic physical exercise which have been published from 2010 to 2016 have been considered.
In future research, impact of fatigue should be considered to prescribe therapeutic exercise in fibromyalgia patients. Validated tools as the Fatigue Impact Scale43 gives measures that allow to identify subjects who could need an individual physical exercise program whose load would be based on their results in a Maximum Ergometric Test.
Conclusion- -
Pain experimented by fibromyalgia patients improve when any physical activity is increased or when this is maintained.
- -
Fibromyalgia patients’ quality of life especially improves with regular performance of therapeutic exercises which require a dynamic mobilization of the patient's body, regardless of load.
- -
Depression, anxiety and mood improve in fibromyalgia patients when they do regular aerobic and flexibility exercises or activities such as aquatic biodance or belly dance.
- -
Quality of sleep also improves when doing regular aerobic exercises combined with relaxation, strength training programs and aquatic biodance, Tai-chi or Qigong.
- -
Supplements may be an interesting therapeutic alternative because of its effectiveness in pain relief and quality of life improvement, however much more studies are needed.
No scholarships or grants have been received for this work.
Conflict of interestsAuthors declare that they don’t have any conflict of interests.
Some of the information in this paper was presented as an oral communication at the FEMEDE Congress, held in Granada, November 24, 2016.

